
 is a skin disorder that occurs due to long-term, repeated...){kind=link}

Solar Elastosis Sun Solar elastosis (actinic elastosis, or elastosis senilis) is a skin disorder that occurs due to long-term, repeated exposure to ultraviolet rays of the sun. The condition is one of the characteristic signs of photoaging and is observed in millions of individuals around the globe, especially those with a fair complexion and a history of intense exposure to the sun. Although solar elastosis is non-cancerous, however, it is a powerful symptom of significant sun radiation damage and can contribute to the future threat of contracting skin cancer.[1]
What is Solar Elastosis?: Solar Elastosis Sun
Solar elastosis is a degenerative process that involves the elastic tissue in the dermis or the deeper layer of the skin under the epidermis. The disease is defined by the formation of excessive, abnormal, degraded elastic tissue that is caused by chronic abuse of the skin by ultraviolet radiation. This literally means destruction of skin elasticity as a result of sun exposure.[2]
How Solar Elastosis Develops
The Normal Skin Structure
The dermis has an organized system of collagen and elastin fibres embedded in a ground substance that contains a lot of glycosaminoglycans, especially hyaluronic acid. Elastin gives the skin its elastic recoil to return to its original position once it is stretched, whereas collagen gives it strength and form.[3]
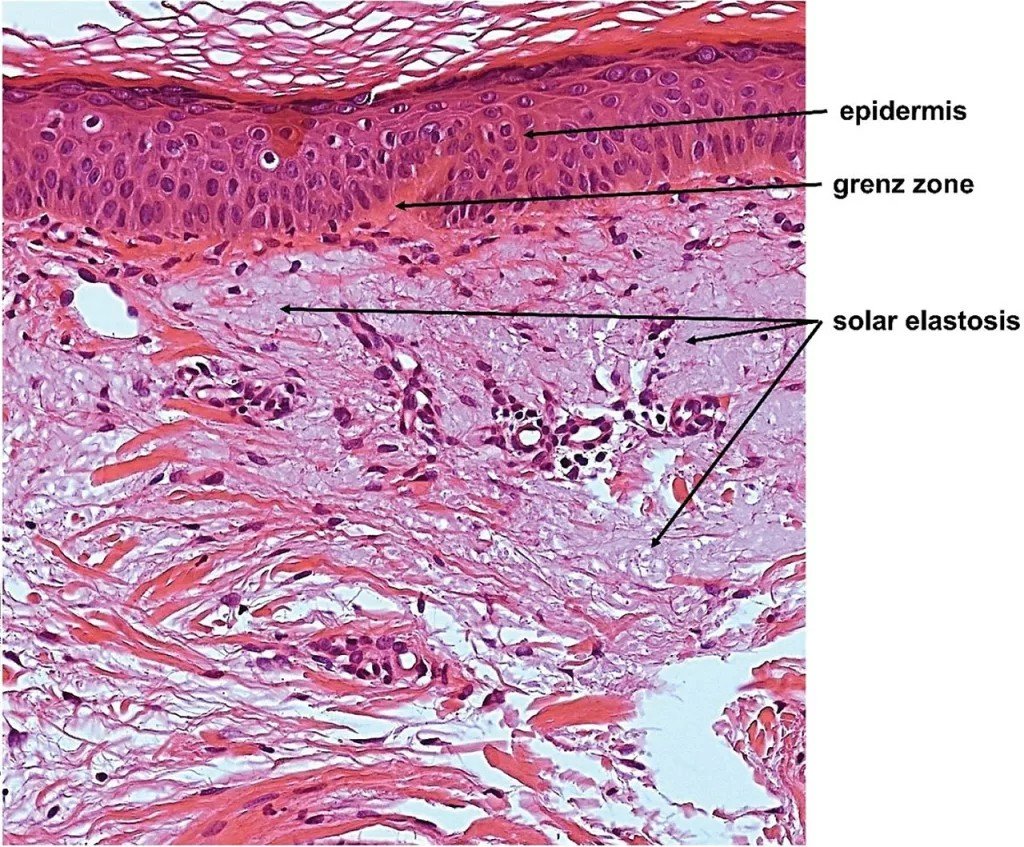
Histopathology of solar elastosis demonstrating disorganized, basophilic elastotic material within the dermis. By Miri Kim and Hyun Jeong Park (2016). “Molecular Mechanisms of Skin Aging and Rejuvenation”. IntechOpen. DOI:10.5772/62983.Creative CommonsAttribution, CC BY 3.0.
The Damaging Effect of UV Radiation
UV radiation, UVA, in particular, initiates the destructive processes in the skin:[4]
- Direct Fiber Damage: UV radiations directly disrupt the collagen and elastin fibers, which affect the structure and elasticity of skin.
- Enzyme Activation: Another way by which UV further breaks down collagen and elastin is by inducing the enzymes (MMPs).
- Abnormal Repair Response: Fibroblasts begin producing disorganized and dysfunctional elastotic material.
- Glycosaminoglycan Accumulation: These are substances that accumulate abnormally on the affected tissue, which leads to a weathered look of the skin.
Progressive Changes Over Time
Solar elastosis worsens with cumulative UV exposure:[5]
- Early Phase: There is a deposition of irregular and thickened elastic fibers.
- Advanced Stage: Fibers become coarse, tangled, and disorganized.
- Microscopic Findings: A basophilic (blue-grey) zone of elastotic material replaces normal collagen, with a “grenz zone” between the dermis and epidermis.
Causes of Solar Elastosis
Primary Cause: Ultraviolet Radiation Exposure
The most important cause of solar elastosis is prolonged and repeated exposure to ultraviolet radiation. Possible sources of these radiations can be:[6]
- Solar radiation is a natural source of vitamin D on the skin, but when the skin has years of sun exposure, it becomes damaged, leading to elastosis.
- Artificial UV ray sources are also damaging to your skin. Such ones may be constant tanning beds and other artificial sources of UV light.
- Jobs: Individuals who spend their time outdoors at the workplace, like farmers, construction workers, fishermen, and athletes, are exposed to UV radiation more often and at a greater rate.
Contributing Factors
The risk of developing solar elastosis may be increased because of the following factors:[7]
Skin Type: Fair-skinned people are more susceptible to UV damage and solar elastosis as compared to darker-skinned people.
Smoking: It accelerates collagen breakdown and contributes to premature photoaging, worsening elastosis.[8]
Medical Conditions: Some medical conditions can increase the risk of developing solar elastosis. Porphyria cutanea tarda is one of them, which increases the photosensitivity.
Immunosuppression: Immunosuppressive treatment also increases sensitivity to UV rays, so it is a risk factor for developing solar elastosis.
Age: Middle-aged and elderly people have longer exposure to sunlight, so they are more prone to it.
Geographic Location: Living at latitudes closer to the equator, where UV radiation is more intense, increases the risk of solar elastosis.
Solar Elastosis Symptoms
Visual Appearance
You can notice the following skin changes due to this disease:[9]
- Skin becomes yellowish and thick. This yellowing of skin occurs because of the deposits of abnormal elastic tissue in the dermis.
- You can see that the affected skin develops a coarse texture with deep wrinkles and furrows.
- Another change you can notice is that you may feel a tough and leathery touch in the skin, having lost its normal softness.
- In some cases, there is a cobblestone-like appearance due to a rough and bumpy texture of skin.
Areas Most Affected
Solar elastosis primarily affects sun-exposed areas of the body, including:[10]
- Face
- Ears
- Back of the neck
- Forearms and hands
- Décolletage (upper chest area)
- Bald scalp
How to Diagnose Solar Elastosis
Clinical Diagnosis
Solar elastosis is diagnosed mainly on its clinical appearance. By examining a yellowish thick skin with too many wrinkles, your dermatologist can detect the issue. You may be asked about all the causes responsible for the disease, like sun exposure, your job nature, use of tanning beds or other artificial UV sources, and history of smoking and medical diseases as well.[11]
Physical Examination
When inspecting a patient, a doctor will observe the changes in the skin and pattern of the affected areas. Other symptoms of sun damage and possible lesions with suspected skin cancers are also valuable.
Confirmatory Testing
Besides clinical assessment, some tests are also suggested to make a certain diagnosis.[12]
Skin Biopsy: A sample of your skin tissue is examined in detail under a microscope. The histological findings of Solar elastosis are presented in the Pathology section.
Special Stains: Pathologists can use special staining methods in order to observe elastic fibers better:
- Verhoeff-Van Gieson stain: Stains make elastic fibers black
- Hematoxylin and eosin (H&E)
Photography: Medical photography can be used to record the appearance of the baseline and monitor the changes over time, especially when treatment is being done.
Differential Diagnosis
There are a few other conditions that may appear like solar elastosis, which should be taken into account:[13]
- Adult colloid milium
- Cutaneous amyloidosis
- Focal mucinoses
- Actinic keratosis
- Basal cell carcinoma
- Sebaceous hyperplasia
- Various forms of dermal tumors
Solar Elastosis Histopathology
The changes that are observed at the microscopic level in solar elastosis can be used to explain the nature of the condition and to influence treatment methods.
Histopathological Features
Solar elastosis under microscopic observation shows the following features:[14]
Early Stage Changes:
- Elastic fiber hyperplasia (fibers have increased in number).
- Abnormal thickening of the elastic fibers in the upper dermis.
- Fiber fragmentation and disorganization are also present.
Advanced Stage Changes:
- In both papillary and reticular dermis, large areas of normal collagen fibers have been replaced by dense, amorphous elastotic material.
- Elastic fibres, which have become thick and curled, form tangled masses.
- Unrefined, untidy elastotic tissue is seen as basophilic (blue-grey) on routine H&E staining.
- Loosely organized fibers and amorphous masses replace the entire dermis.
Special Features:
- Grenz zone: A thin strip of normal appearing collagen between the elastotic material and the epidermis.
- Mild perivascular and periadnexal lymphocytic infiltrate
- The existence of glycosaminoglycans (hyaluronic acid and versican) on elastotic material.
Comparison with Normal and Aged Skin
| Feature | Normal Skin | Intrinsically Aged Skin | Solar Elastosis |
|---|---|---|---|
| Elastic Fiber Content | Organized, functional fibers | Reduced the disintegration of elastin and fiber | Increased abnormal elastic material |
| Collagen Structure | Strong, organized bundles | General atrophy; reduced collagen | Collagen is replaced by an elastic material |
| Dermal Thickness | Normal | Thinning | Variable; often thickened |
| Fiber Organization | Regular, parallel arrangement | Disorganized but not tangled | Tangled as well as severely disorganized |
| Microscopic Appearance | Pink (eosinophilic) fibers | Reduced, fragmented fibers | Blue-purple (basophilic) elastotic material |
| Location of Changes | N/A | Generalized dermal atrophy | Concentrated in sun-exposed areas |
Solar Elastosis vs Actinic Keratosis
Both solar elastosis and actinic keratosis are the results of chronic sun exposure but they are different conditions with different characteristics and implications.[15]
Key Differences
| Aspect | Solar Elastosis | Actinic Keratosis |
|---|---|---|
| Nature of Condition | Dermal elastic tissue degenerative change | Precancerous epidermal lesion |
| Primary Location | Dermis (deeper skin layer) | Epidermis (outer skin layer) |
| Cancer Risk | Not precancerous itself, but indicates sun damage | Precancerous; can progress to squamous cell carcinoma |
| Appearance | Leathery, thick, wrinkled skin, which is yellow. | Rough, scaly patches or plaques; red, pink, or flesh-colored |
| Texture | Smooth to cobblestone surface; deep wrinkles | Sandpaper-like texture that is rough as well |
| Symptoms | Usually asymptomatic | May be tender, itchy, or bleeding |
| Size | Involves big portions of uncovered sun-exposed skin | Single discrete lesions, most of which are less than 1-2 cm |
| Cell Changes | Abnormal elastic tissue accumulation | Atypical keratinocytes with dysplasia |
| Treatment Priority | Aesthetic enhancement and aversion to additional harm | Medical necessity to avoid the development of cancer. |
Solar Elastosis Treatment
The primary aim of treatment is twofold: to prevent further photodamage and improve the cosmetic appearance of elastotic skin.
Prevention: The Foundation of Treatment
Strict sun protection is needed to avoid the exacerbation of solar elastosis. This involves using daily broad-spectrum sunscreen (SPF 30+), reapply after every two hours, as well as using protective clothing and avoiding the sun. In addition, stop smoking, eat healthy foods with lots of vegetables, and keep hydrated, which keeps the skin healthy.
Topical Treatments
Some tropical treatments have the best results in treating the disease, for example:
Retinoids: The Gold Standard Treatment
Topical retinoids have the best effects in reversing solar elastosis. They act through the stimulation of collagen production, cell renewal, and enhancement of skin texture. They do not cure elastosis but improve surface appearance.[16]
Prescription Options:
- Tretinoin: Begin with 0.025 percent cream, which is applied once a night, and increase in strength.
- Tazarotene: A potent option (0.05% – 0.1%).
- Adapalene: A 0.1% retinoid.

The exact pea-sized dose of retinoids to use.
It is essential to control the expectations and possible side effects when initiating a retinoid. There is preliminary irritation, such as erythema, peeling, and drying. To reduce this, use only a pea-sized amount on dry skin; also, apply a moisturizer before retinoids. It requires patience because the immediate results of the skin texture and elasticity may take 3-6 months to view
Alpha Hydroxy Acids (AHAs):
Alpha Hydroxy Acids(AHAs): Glycolic acid may be an addition to retinoid treatment. Begin with a low concentration (e.g., 10) and use twice or three times a week in the morning, and increase in strength gradually as you can tolerate, and 20 is usually the limit.[17]
Other Topical Agents:
Immunodefiners such as Imiquimod, Tacrolimus ointment, and topical estrogen in post-menopausal women can also offer some benefits. Imiquimod and tacrolimus are not standard treatments for solar elastosis, but may incidentally improve sun-damaged skin when used for other indications. Also, the antioxidants (e.g., Vitamin C) and growth factor/peptide preparations can be used to prevent additional harm and promote skin rehabilitation.[18]
Laser and Light-Based Treatments
Laser and light therapies are also most effective in solar elastosis and these techniques operate by destroying the damaged skin and activating the formation of new collagen.
Ablative Lasers (Gold Standard):
- CO2 Laser: The best option when it comes to moderate to severe cases. It evaporates the burnt skin, causing extensive collagen regeneration. Ablative ones provide more dramatic results and take 2-3 weeks to restore, whereas Fractional types recover in less time (approximately 1 week).[19]
- Erbium Laser: Treats superficial to moderate damage with less thermal effect and shorter downtime than CO2.
Non-Ablative & Light Therapies (Less Downtime):
- Non-Ablative Fractional Lasers (e.g., Fraxel): Penetrate deeply without damaging the surface, requiring multiple sessions but with minimal downtime (a few days).[20]
- Intense Pulsed Light (IPL): This laser mainly enhances sun-related pigments and redness and is frequently used together with other types of lasers in a bid to achieve a more holistic outcome.
Injectable & Procedural Treatments
These are used to treat the impact of solar elastosis by replacing skin volume, collagen, or resurfacing the skin.[21]
Injectables:
Dermal fillers, collagen stimulators, and Botox can soften wrinkles, but do not treat elastosis itself but they improve cosmetic appearance.
- Dermal Fillers (e.g., Juvederm, Radiesse) fill up the lost volume and deep wrinkles to make them smooth immediately.
- Collagen-Stimulators (e.g., Sculptra) are used slowly to restore the natural collagen deposits of the skin, and their effects may last more than two years.
- Neurotoxins (e.g., Botox) loosen wrinkles of the muscles and should be used together with other therapies.
Resurfacing & Remodeling Procedures:
- Chemical Peels (e.g., TCA) peel off the old layers of skin to enhance the skin texture and promote the growth of new collagen.[22]
- Microneedling Radiofrequency is a micro-injury combined with deep heat to tighten the skin and increase collagen with minimal downtime.
- Dermabrasion is a mechanical resurfacing technique of the skin, but it is now usually replaced by superior lasers.
How Long Does Solar Elastosis Take to Develop, and Can It Be Reversed?
Solar elastosis is an age-related process, starting to accumulate UV damage since childhood and commonly not showing any visible effects until the age of 40 or more, but again, it depends upon the sun exposure, skin type, and lifestyle habits such as smoking. Although the resulting damage to the elastic tissue is irreversible and cannot be fully recovered.[23]
The appearance can be dramatically improved with the treatments that promote the production of new collagen, diminish wrinkles, and improve the texture of the skin. The most essential thing is that the strict, daily use of sun protection measures ensures that no subsequent damage will be caused.
Conclusion
To conclude, solar elastosis is a permanent disorder resulting in a leathery, wrinkled look on the skin due to the breakdown of the supportive structure caused by the sun. The damage is permanent, but its external manifestations may be greatly enhanced with medications such as retinoids and laser treatments. Consistent and strict sun protection is, however, the most critical step in ensuring that the condition does not deteriorate.
References
[1] Warren R, Gartstein V, et al. Age, sunlight, and facial skin: a histologic and quantitative study. J Am Acad Dermatol. 1991;25:751-760.
[2] Oikarinen A. The aging of skin: chronoaging versus photoaging. Photodermatol Photoimmunol Photomed. 1990;7(1):3-4.
[3] Varani J, Dame MK, Rittie L, et al. Decreased collagen production in chronologically aged skin: roles of age-dependent alteration in fibroblast function and defective mechanical stimulation. Am J Pathol. 2006;168(6):1861-1868.
[4] Kadoya K, Sasaki T, Kostka G, et al. Fibulin-5 deposition in human skin: decrease with ageing and ultraviolet B exposure and increase in solar elastosis. Br J Dermatol. 2005;153(3):607-612.
[5] Bouissou H, Pieraggi M-T, Julian M, Savit T. The elastic tissue of the skin: a comparison of spontaneous and actinic (solar) aging. Int J Dermatol. 1988;27:327-335.
[6] Gilchrest BA. Skin aging and photoaging: an overview. J Am Acad Dermatol. 1989;21(3 Pt 1):610-613.
[7] Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124(6):869-871.
[8] Frances C. Smoker’s wrinkles: epidemiological and pathogenic considerations. Clin Dermatol. 1998;16(5):565-570.
[9] Milian G. Citrine skin: a clinical sign of extensive degenerative elastosis in actinically damaged skin. Arch Dermatol. 1929;19:687-692.
[10] Nürnberger F, Schober E, Marsch WC, et al. Actinic elastosis in black skin: a light- and electronmicroscopic study. Arch Dermatol Res. 1978;262:7-16.
[11] Kossard S, Anderson P, Davies A, Cooper A. Histological evaluation of the effect of 0.05% tretinoin in the treatment of photo damaged skin: geographic differences in elastosis in baseline biopsies. Australas J Dermatol. 1993;34(3):89-95.
[12] Suwabe H, Serizawa A, Kajiwara H, et al. Degenerative processes of elastic fibers in sun-protected and sun-exposed skin: immunoelectron microscopic study. J Cutan Pathol. 1999;26(1):25-31.
[13] Hsu CK, Hsu MM, Lee JY. Desmoplastic melanoma: a clinicopathologic study of 14 cases in Taiwanese patients. J Am Acad Dermatol. 2004;50(3):393-397.
[14] Mitchell RE. Chronic solar dermatosis: a light and electron microscopic study of the dermis. J Invest Dermatol. 1967;48:203-220.
[15] Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet. 1988;1(8589):795-797.
[16] Kligman AM, Grove GL, Hirose R, Leyden JJ. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15(4 Pt 2):836-859.
[17] Van Scott EJ, Yu RJ. Hyperkeratinization, corneocyte cohesion, and alpha hydroxy acids. J Am Acad Dermatol. 1984;11(5 Pt 1):867-879.
[18] Wolf JE Jr, Taylor JR, Tschen E, Kang S. Topical 3.0% diclofenac in 2.5% hyaluronan gel in the treatment of actinic keratoses. Int J Dermatol. 2001;40(11):709-713.
[19] Fitzpatrick RE, Goldman MP, Satur NM, Tope WD. Pulsed carbon dioxide laser resurfacing of photoaged facial skin. Arch Dermatol. 1996;132(4):395-402.
[20] Goldberg DJ. Non-ablative subsurface remodeling: clinical and histologic evaluation of a 1320-nm Nd:YAG laser. J Cutan Laser Ther. 1999;1(3):153-157.
[21] Vleggaar D, Bauer U. Facial enhancement and the European experience with Sculptra (poly-L-lactic acid). J Drugs Dermatol. 2004;3(5):542-547.
[22] Monheit GD, Chastain MA. Chemical peels. Facial Plast Surg Clin North Am. 2001;9(2):239-255.
[23] Yaar M, Gilchrest BA. Photoageing: mechanism, prevention and therapy. Br J Dermatol. 2007;157(5):874-887.