
 or vesicoureteric reflux is a condition where urine flows backward from the bladder...){kind=link}

Vesicoureteral Reflux Risks Vesicoureteral reflux (VUR) or vesicoureteric reflux is a condition where urine flows backward from the bladder toward the kidneys instead of flowing in the normal direction out of the body. This backward flow happens through the ureters (tubes connecting the bladder to the kidneys). It is most commonly suspected after a febrile urinary tract infection (UTI) in a child, after abnormal kidney findings on prenatal ultrasound, or when there is a family history of VUR.
VUR is most common in infants and children. Early recognition and proper treatment reduce the risk of kidney scarring and help ensure excellent outcomes.
Understanding Vesicoureteral Reflux Symptoms: Vesicoureteral Reflux Risks
As young children can’t explain their pain, identifying the symptoms of VUR may be difficult for them. The first sign is often repeated urinary tract infections, sometimes accompanied by fever, especially in infants.
Common Symptoms in Children:
The following symptoms are seen in children with VUR:
- Repeated urinary tract infections (UTIs)
- Fever with no obvious reason- a special concern in infants
- Pain or burning during urination – Older children can tell this problem.
- Urgency and frequency of urine (Can lead to Bedwetting)
- Cloudy or smelly urine
- Pain in the abdomen or moving to the back – it may show kidney involvement
- Some children may also present with hematuria, which can be visible to the parents or detected only on routine urinalysis.
Symptoms in Toddlers & Infants:
Younger children who cannot tell their symptoms may show:
- Unexplained fussiness or irritability
- Poor appetite or loss of appetite
- Inability to thrive or gain weight
- Chronic diaper rash in the genitalia
- Changes in urination patterns
- Vomiting with fever (can suggest a kidney infection)
Not all children with VUR have symptoms. Milder cases may only be discovered during prenatal ultrasounds or through screening when a sibling has been diagnosed.
What Causes Vesicoureteral Reflux?
Normally, some valves regulate urine flow from the kidneys to the bladder. VUR is found when these valves are non-functional between the bladder and the ureter.
There are two types of VUR depending on the cause:
Primary Vesicoureteral Reflux:
Primary VUR is the most common type that is present at birth, as a result of a developmental problem. In a healthy urinary system, the ureter enters the bladder at an angle and forms a natural one-way valve. When your child’s bladder is full of urine, this valve prevents urine from flowing backwards.
In primary VUR, this valve mechanism is immature or is formed incorrectly, allowing urine to flow backwards from the bladder into the ureter and possibly up to the kidney. This condition is often a transient condition that improves as the child grows up and his or her urinary anatomy matures.
Secondary Vesicoureteral Reflux:
Secondary VUR develops because of some other problems that cause a higher pressure in the bladder or obstruct the flow of urine. Common causes include:
- Bladder dysfunction – Problems with how the bladder empties
- Urethral obstructions – Obstruction (blockage) in the tube through which urine leaves the body
- Neurological problems – The problems with the nerve control of the bladder.
- Prolonged constipation can strain the bladder.
What Risk Factors Increase the Chances of VUR?
Several factors increase the likelihood of developing VUR:
- Family history – VUR is a family-inherited ailment.
- Gender – Girls are more commonly affected, except in newborns, where the incidence in boys is higher
- Race – More common in Caucasian children
- Other UTI abnormalities
How is VUR Diagnosed?.
Vesicoureteral reflux diagnosis usually starts when a child develops a urinary tract infection (especially one that involves the kidneys, known as pyelonephritis), or in a young child where UTIs are uncommon.
Initial Evaluation:
Your child’s doctor will start with:
- Medical history that includes any previous UTIs or family history of VUR
- Physical examination to check for any signs of kidney problems or other abnormalities.
- Urine tests – To see an infection and to detect other abnormalities
Imaging Studies:
Several tests can be used to diagnose VUR:
Voiding Cystourethrogram (VCUG)
The gold standard testing for the diagnosis of VUR is the VCUG. During this procedure:
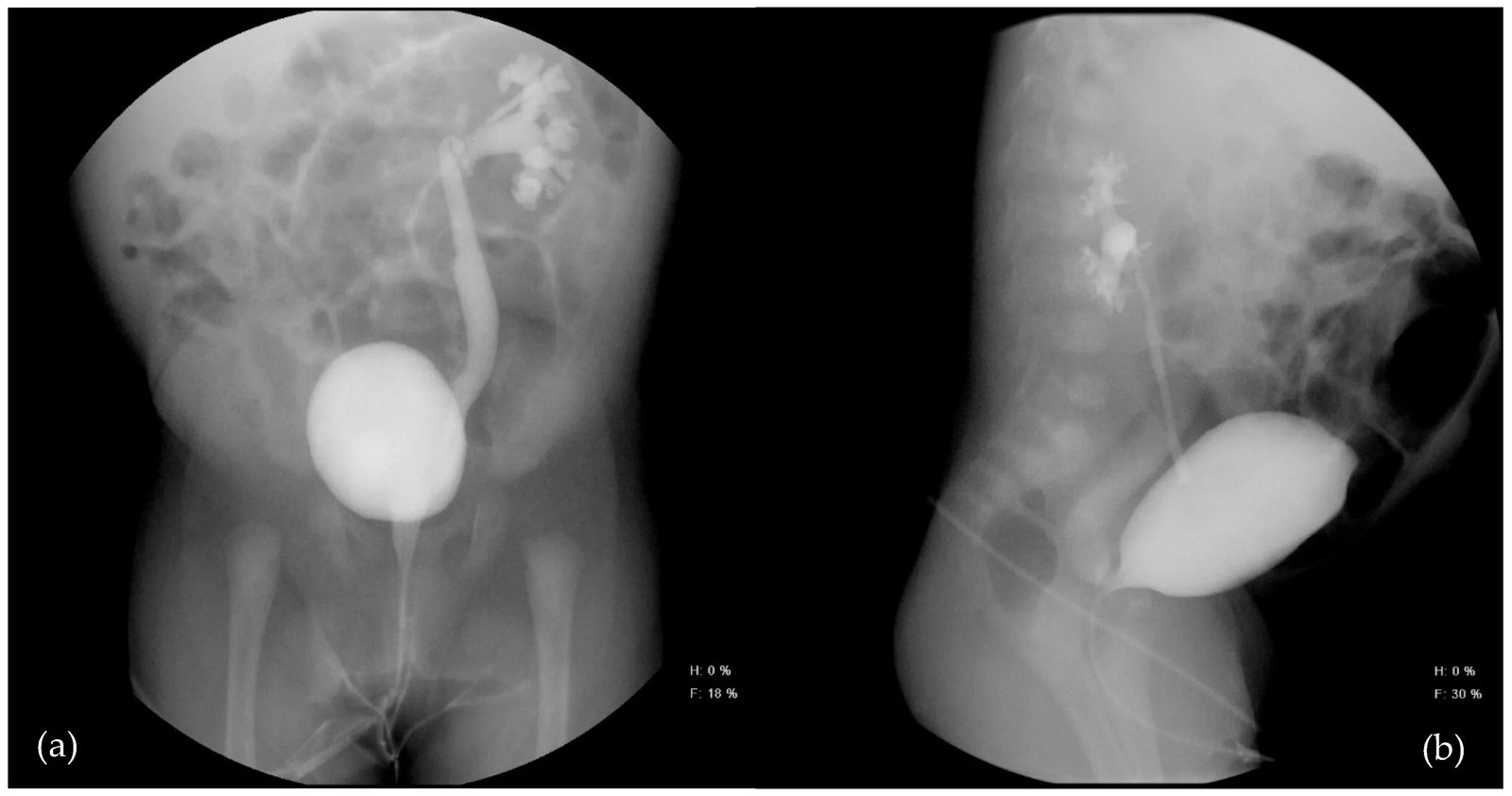
Voiding cystourethrogram: (a) (left kidney, anteroposterior view): Grade IV vesicoureteral reflux is observed, with dilation of the ureter, renal pelvis, and calyces. Partial preservation of the papillary impressions is noted; (b) (right kidney, lateral view): Grade V vesicoureteral reflux is evident, with severe dilatation of the pelvicalyceal system and a tortuous ureter. Loss of normal calyceal morphology and obliteration of the papillary impressions are observed. Adapted from 8805.MDPI. Licensed under CC BY 4.0.
- A thin catheter is inserted into the bladder of your child
- Contrast dye that is used to fill the bladder
- Take X-ray images during the filling and emptying of the bladder.
- The test indicates whether urine flows back into the ureters
While this test can be uncomfortable, it is the most accurate way of determining the presence and severity of VUR.
Ultrasound
Kidney ultrasound is often the first imaging test because it’s:
- Non-invasive and painless
- Doesn’t use radiation
- Can detect kidney swelling (hydronephrosis)
- Can identify other structural abnormalities
However, ultrasound alone cannot definitively diagnose VUR.
Nuclear Medicine Scans
DMSA (dimercaptosuccinic acid) scans can be used to:
- Detect kidney scarring
- Evaluate individual kidney function
- Monitor changes over time
Understanding Vesicoureteral Reflux Grading
Vesicoureteral reflux grading is crucial for determining treatment approaches and predicting outcomes. The medical community uses a standardized 5-grade system based on how far the urine backs up and how much the urinary tract is dilated (widened).
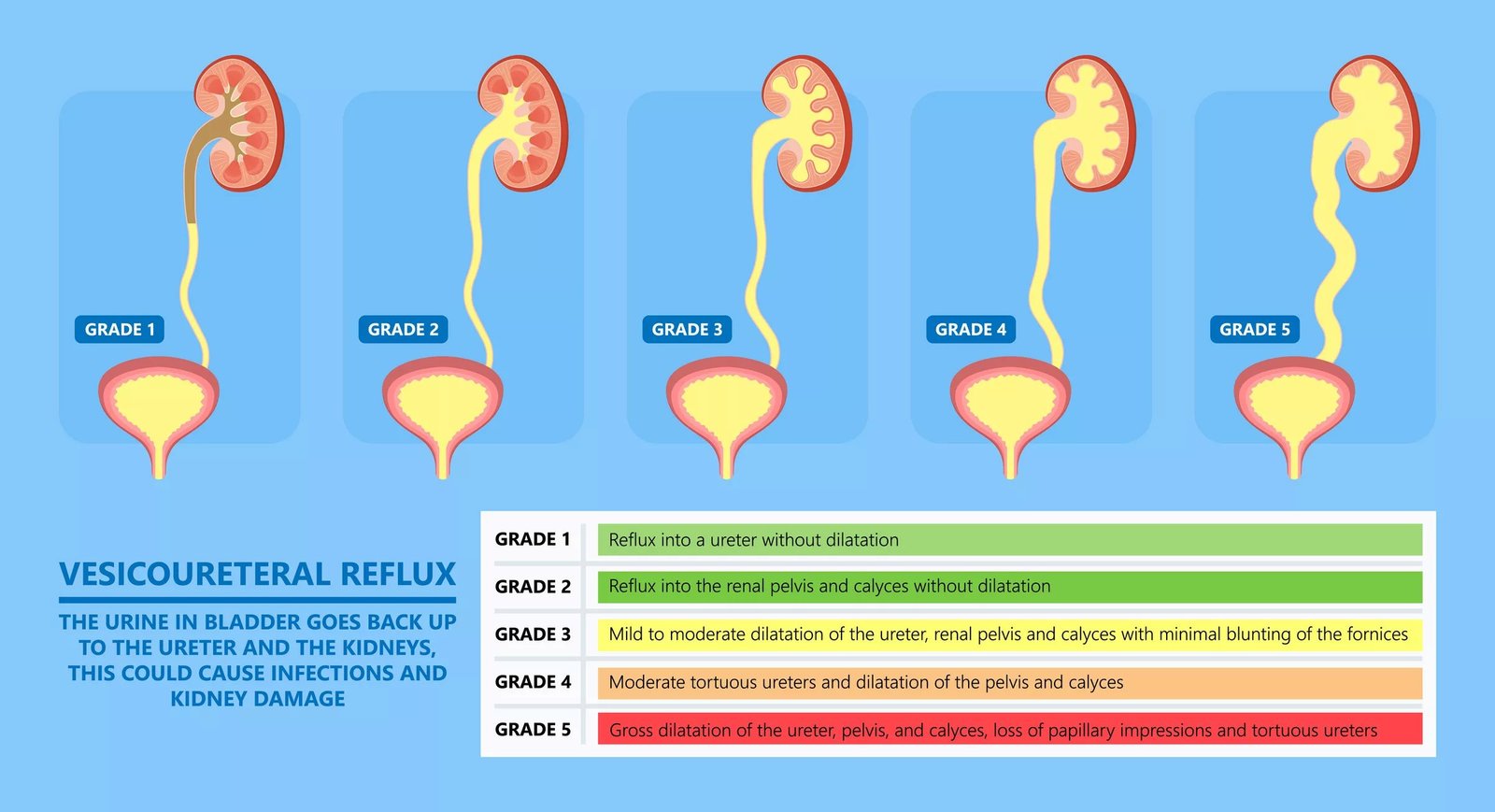
The image shows grades of VUR
The VUR Grading System:
In Grade I (Mild)
- Urine backs up only into the lower portion of the ureter
- No dilation of the ureter or kidney structures
- Often resolves on its own as the child grows
Grade II (Mild to Moderate)
- Urine backs up all the way to the kidney
- Minimal or no dilation of the ureter or kidney collecting system
- Good chance of spontaneous resolution
Involvement in Grade III (Moderate)
- Mild to moderate dilation of the ureter
- Mild dilation of the kidney collecting system
- May resolve with time, but monitoring is important
Grade IV (Moderate to Severe)
- Moderate dilation of the ureter
- Moderate dilation of the kidney collecting system
- Less likely to resolve spontaneously; may require surgical intervention
Grade V (Severe)
- Severe dilation and tortuosity (twisting) of the ureter
- Significant dilation of the kidney collecting system
- Typically requires surgical treatment
Why Grading Matters?
The grade of VUR helps doctors:
- Predict whether the condition will improve on its own
- Determine the appropriate treatment approach
- Assess the risk of kidney damage
- Plan follow-up care and monitoring
Vesicoureteral Reflux Treatment Options
Vesicoureteral reflux treatment approaches vary significantly based on the grade of VUR, your child’s age, the frequency of infections, and other individual factors. The primary goals of treatment are to prevent urinary tract infections and protect the kidneys from damage.
Conservative Management:
For many children, especially those with lower-grade VUR, a “watchful waiting” approach is appropriate.
Antibiotic Prophylaxis
Prophylactic antibiotics involve giving your child a low-dose antibiotic daily to prevent UTIs while waiting for the VUR to resolve naturally. This approach typically includes:
- Daily low-dose antibiotics (commonly trimethoprim-sulfamethoxazole or nitrofurantoin)
- Regular urine monitoring to check for breakthrough infections
- Periodic imaging to assess whether the VUR is improving
- Bladder and bowel management to optimize urinary health
Supporting Measures
Additional conservative measures include:
- Encouraging complete bladder emptying – Teaching proper voiding techniques
- Managing constipation – As constipation can worsen VUR
- Maintaining good hygiene – Especially important for girls
- Ensuring adequate fluid intake – To dilute urine and reduce infection risk
Surgical Treatment Options:
Surgery may be recommended for children with higher-grade VUR, recurrent breakthrough infections despite antibiotics, or evidence of kidney scarring.
Endoscopic Treatment (DEFLUX Injection)
This minimally invasive procedure involves:
- Outpatient surgery under general anesthesia
- Injection of a bulking agent (DEFLUX) near the ureter opening
- Creation of an artificial valve to prevent urine backflow
- Quick recovery with minimal discomfort
The success rate is good for lower-grade VUR but may be less effective for higher grades.
Open Surgical Repair (Ureteral Reimplantation)
This more extensive surgery involves:
- Creating a new pathway for the ureter into the bladder
- Establishing a longer tunnel to create an effective valve mechanism
- High success rates (over 95%) for preventing VUR
- Longer recovery time, but definitive treatment
Minimally Invasive Approaches
Newer techniques include:
- Laparoscopic reimplantation – Using small incisions and a camera
- Robot-assisted surgery – For enhanced precision
- Faster recovery compared to traditional open surgery
Potential Complications of Vesicoureteral Reflux
Understanding vesicoureteral reflux complications helps emphasize the importance of proper monitoring and treatment. While VUR itself doesn’t typically cause symptoms, the complications from untreated or inadequately managed VUR can be significant.
Kidney Scarring (Renal Scarring):
The most serious complication of VUR is kidney scarring, which can result from:
- Recurrent kidney infections (pyelonephritis)
- High-grade VUR with significant pressure on the kidney tissue
- Delayed or inadequate treatment of urinary tract infections
Kidney scarring is permanent and can lead to:
- Reduced kidney function
- High blood pressure later in life
- Pregnancy complications in women
- Chronic kidney disease in severe cases
Hypertension (High Blood Pressure):
Renal scarring can lead to high blood pressure because:
- Damaged kidneys may not regulate blood pressure effectively
- The risk increases with the extent of scarring
- Regular blood pressure monitoring is essential for children with a history of VUR
Chronic Kidney Disease:
In severe cases with extensive bilateral (both kidneys) scarring:
- Progressive kidney function decline may occur
- End-stage kidney disease is rare but possible
- Early detection and treatment significantly reduce this risk
Recurrent Infections:
Without proper management, children may experience:
- Frequent UTIs that are difficult to treat
- Antibiotic resistance from repeated treatments
- Impact on quality of life and normal childhood activities
Vesicoureteral Reflux Prognosis
The vesicoureteral reflux prognosis is generally excellent, especially when the condition is diagnosed early and managed appropriately. Understanding the outlook can provide much-needed reassurance for worried parents.
Natural Resolution:
Many children with VUR will outgrow the condition naturally:
- Grade I and II VUR resolves in 80-85% of children
- Grade III VUR resolves in about 50-60% of children
- Grade IV and V VUR have lower spontaneous resolution rates (15-20%)
- Resolution typically occurs by age 5-7 years
Treatment Success Rates:
When surgical intervention is needed:
- Endoscopic treatment success rates range from 70 to 90%
- Open surgical repair has success rates exceeding 95%
- Repeat procedures may be necessary in some cases
- Most children achieve complete resolution of VUR
Long-term Outcomes:
With proper management:
- Most children grow up with normal kidney function
- The risk of kidney damage is significantly reduced with appropriate treatment
- Quality of life is typically excellent
- Future pregnancies are generally uncomplicated
Factors Affecting Prognosis:
Several factors influence outcomes:
- Age at diagnosis – Earlier detection generally leads to better outcomes
- Grade of VUR – Lower grades have better spontaneous resolution rates
- Prompt treatment of UTIs – Reduces risk of kidney scarring
- Family compliance with treatment recommendations
Conclusion
Vesicoureteral reflux may seem overwhelming when you first learn about your child’s diagnosis, but it’s important to remember that this is a well-understood and highly treatable condition. With advances in medical understanding and treatment options, the vast majority of children with VUR go on to live completely normal, healthy lives.
The key to successful management lies in working closely with your healthcare team, following treatment recommendations consistently, and maintaining vigilance for signs of urinary tract infections. Whether your child’s VUR resolves naturally or requires surgical intervention, the prognosis is excellent when the condition is properly managed.
Remember that you’re not alone in this journey. Your pediatric urologist and healthcare team are there to guide you through every step, from initial diagnosis through treatment and long-term follow-up. With their expertise and your dedication to your child’s care, you can feel confident that your child will have the best possible outcome.
References
[1] Mattoo, T. K. (2007). Vesicoureteral reflux and reflux nephropathy.Advances in Chronic Kidney Disease, 14(4), 336–344.
[2] Skoog, S. J., Peters, C. A., Arant, B. S., Copp, H. L., Elder, J. S., Hudson, R. G., Khoury, A. E., & Pope, J. C. (2010). Pediatric vesicoureteral reflux guidelines panel summary report.The Journal of Urology, 184(3), 1134–1144.
[3] Routh, J. C., Inman, B. A., & Reinberg, Y. (2010). Vesicoureteral reflux: Current trends in diagnosis, screening, and treatment.European Urology, 58(4), 651–659.
[4] Copp, H. L., & Nelson, C. P. (2012). Clinical presentation and evaluation of vesicoureteral reflux.Current Opinion in Pediatrics, 24(2), 207–214.
[5] Mattoo, T. K., & Mathews, R. (2003). Vesicoureteral reflux and urinary tract infection: evolving practices and new concepts.Pediatric Nephrology, 18(9), 922–930.
[6] Estrada, C. R., & Passerotti, C. C. (2009). Imaging strategies for vesicoureteral reflux.Urologic Clinics of North America, 36(2), 213–224.
[7] Lebowitz, R. L., Olbing, H., Parkkulainen, K. V., Smellie, J. M., & Tamminen-Möbius, T. E. (1985). International system of radiographic grading of vesicoureteric reflux.Pediatric Radiology, 15(2), 105–109.
[8] Puri, P., & Chertin, B. (2009). Treatment of vesicoureteral reflux by endoscopic injection of dextranomer/hyaluronic acid copolymer (Deflux): A multicenter experience.The Journal of Urology, 182(4), 1534–1539.
[9] Smellie, J. M., Jodal, U., Lax, H., Möbius, T. T., Hirche, H., Olbing, H., … & Wennerström, M. (2001). Outcome at 10 years of severe vesicoureteric reflux managed medically: International reflux study in children.Pediatric Nephrology, 16(12)
[10] Ardissino, G., Dacco, V., Testa, S., Bonaudo, R., Claris-Appiani, A., Taioli, E., … & Marra, G. (2004). Epidemiology of chronic renal failure in children: Data from the ItalKid project.Pediatrics, 114(4), e475–e482.
[11] Sillen, U., & Brandstrom, P. (2005). The Swedish reflux trial in children: Management, results, and long-term follow-up.Pediatric Nephrology, 20(2), 165–170.
[12] Olbing, H., & Smellie, J. M. (2002). Long-term prognosis in children with vesicoureteral reflux.Pediatric Nephrology, 17(12), 1022–1031.
[13] Finnell, S. M. E., Carroll, A. E., & Downs, S. M. (2011). Technical report—Diagnosis and management of an initial UTI in febrile infants and young children.Pediatrics, 128(3), e749–e770.