
, also known as Paradoxical vocal fold movement, inducible laryngeal obstruction, or exercise-induced laryngeal...){kind=link}

Vocal Cord Dysfunction (VCD), also known as Paradoxical vocal fold movement, inducible laryngeal obstruction, or exercise-induced laryngeal obstruction, is a breathing disorder in which the vocal folds inappropriately move toward the midline during inhalation or exertion. This narrowing of the airway prevents the vocal cords from opening fully, which leads to noisy breathing, throat tightness, and voice changes. Unlike asthma, the problem does not arise from inflammation of the lungs or bronchi, but from abnormal motion of the vocal cords themselves.
Studies have shown that VCD may be present in up to 2–3% of certain patient groups, and that it accounts for as many as 2.5–22% of unexplained dyspnea cases seen in emergency care. It is also more frequently diagnosed in women and adolescents, especially young athletes with exercise-induced laryngeal obstruction (EILO).
There is no cure for it, and doctors provide symptomatic management by minimizing the triggers of the obstruction. Patients suffering from frequent episodes of VCD can learn to prevent them from happening with a doctor’s guidance.
How do your Vocal Cords work?
To understand what VCD is, it is important to know about the anatomy of your voice box and the vocal cords. Your vocal cords are basically two muscular bands, located inside your voice box, i.e., larynx.
These bands/folds of muscle alter the pathway of the passing air by coming close and meeting in the middle. The vibration of the muscular folds gives you your voice and the ability to alter it (yell, sing, yodel, etc.). They move apart (abduct) when you inhale to allow air into your lungs, and they come together (adduct) to produce voice when you speak, sing, cough, or clear your throat.
In VCD, instead of opening during inhalation, the cords close partially, narrowing the airway. This faulty movement produces the characteristic symptoms of the disorder.
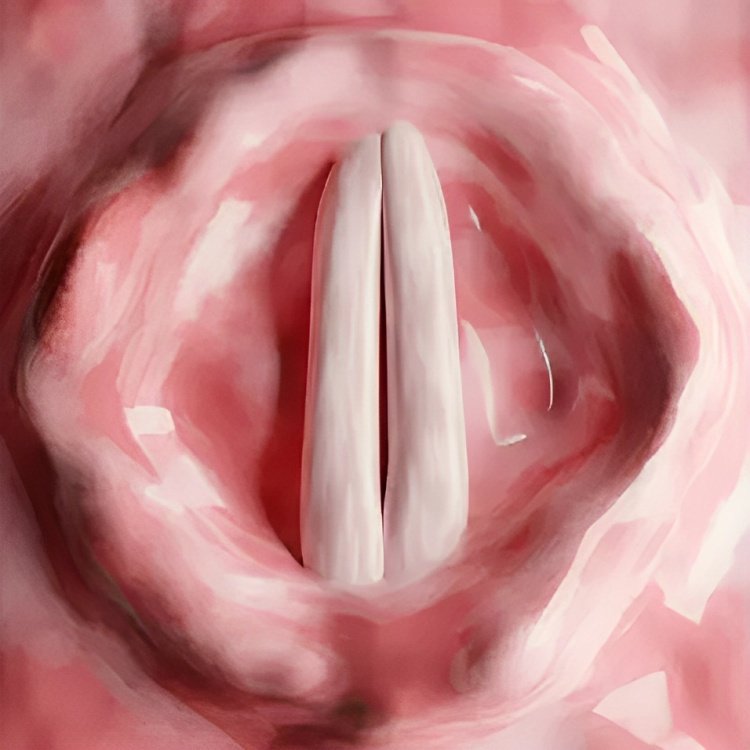
Anatomy of the vocal cords
Vocal Cord Dysfunction Symptoms
Patients suffering from paradoxical vocal movement often complain of having the following symptoms
Lump In Throat:
Sometimes, patients with vocal cord dysfunction experience globus, i.e., a sensation of a lump in the throat. The mass is mostly painless. According to clinical literature, common symptoms of VCD include globus, dysphagia, voice changes, and throat tightness, etc.It was revealed in a study that several patients with a sensation of a throat lump have underlying motion abnormalities of the vocal cords.
Stridor:
Noisy breathing or stridor is a salient feature of underperforming vocal cords. This happens because of the partial opening of the cords during inhalation of breath, which leads to vibration of the bands. Clinicians attribute the stridor to inappropriate adduction (movement of muscle bands towards the midline) of the cords during inspiration. Thus, the most common presentation of this adduction is stridor followed by refractory asthma.
Throat Tightness:
Paradoxical vocal fold movement can induce a feeling of throat tightness. The incomplete opening of the vocal folds makes patients feel some tightness. These feelings are attributed to glottic laryngeal narrowing caused by the disorder.
Shortness Of Breath:
Breathing difficulties accompany feelings of laryngeal tightness and stridor. Inducible laryngeal obstruction is known to cause breathing impairments in patients.Numerous patients visit the ER due to breathing incapability and stridors. Athletes suffering from the disorder report having dyspnea on exertion. Moreover, there are sudden episodes of shortness of breath that impact the quality of life of patients.
Voice Hoarseness:
Another issue that patients often experience due to laryngeal constriction is voice hoarseness. Dysphonia (or hoarseness) is frequently seen in individuals with VCD. It is characterized by the production of strained sounds that have altered pitch and volume. In many cases, doctors track the progress of treatment by noticing the changes in levels of hoarseness. Several patients are unable to speak loudly, which becomes a source of discomfort.
Coughing & Irritation:
Several patients have a chronic cough associated with underlying vocal cord dysfunction. Studies show that patients with VCD have an increased cough frequency, i.e., 17.3 coughs/hour. Thus, it is regarded as a significant symptom of the disorder. This highlighting feature is mostly seen in conjunction with breathing pattern abnormalities. Moreover, you might also feel irritation in your throat and a subsequent constant urge to clear that out. This leads to an increase in cough frequency.
Severe obstructions can seriously compromise your breathing. The initial presentation of such a condition can be dizziness and lightheadedness. You must immediately report to the hospital if you are experiencing dizziness or lightheadedness following an episode of noisy breathing!
Unlike asthma, symptoms of ILO do not subside or alleviate with the use of bronchodilators and corticosteroids because this issue is the outcome of midline movement of the vocal folds and not due to inflammation of the respiratory tract.
Vocal Cord Dysfunction Causes
Abduction of the vocal cord muscles allows unimpeded flow of air during inspiration. However, in this disorder, there is adduction that hinders the airflow, leading to problems.
The exact cause of ILO is unknown. However, based on patient experiences, experts have identified different triggers for paradoxical vocal cord movement.
Vocal Cord Dysfunction Triggers:
The most common triggers of VCD are discussed below:
Exercise
Hectic activity and exercise can act as a trigger for vascular cord dysfunction in some people. Young athletes often suffer from exercise-induced laryngeal obstruction. According to patient accounts, intermittent dysnea occurs in athletes following exercise. This exercise-induced laryngeal obstruction is attributed to vocal fold adduction. It should be kept in mind that exercise-induced bronchoconstriction and exercise-induced asthma are different disorders requiring different treatment strategies. Therefore, they should not be confused with laryngeal obstruction.

Hard athletic training can trigger vocal cord dysfunction
Studies show that exercise-induced dyspnea can disrupt an athlete’s performance and participation.
Gastrointestinal Reflux Disease (GERD)
The reflux of acidic stomach contents into the larynx can pose significant problems. Multiple studies have highlighted the impact of gastrointestinal reflux disease on the larynx and voice quality. Vocal cords irritated and inflamed by the activity of the stomach acid can trigger vocal cord dysfunction. However, GERD control doesn’t completely resolve symptoms of VCD despite it being a trigger for the obstruction.
Respiratory Tract Infection
Bacterial infestation of your upper respiratory tract can impact the performance of your vocal cords. Factors like postnasal drainage and upper respiratory tract infections are believed to act as triggers for VCD. Clinicians found that the incidence of VCD increased during the COVID-19 pandemic. A study revealed that the incidence increased from 5.2% in 2019 (before COVID) to 10.3%, indicating a relation between upper respiratory tract infections and vocal cord dysfunction.
Irritants
Irritant-induced vocal cord dysfunction is not uncommon. Different chemical irritants that can trigger inducible laryngeal obstruction include:
- Ammonia
- Cold and dry air
- Chlorine (in swimming pools)
- Bleaching chemicals
- Cigarette smoke/fumes
- Pungent smells or even strong fragrances
These irritants are known to cause vocal cord abnormalities like palsy that present with stridor. This type of inducible laryngeal obstruction usually develops within 24 hours of exposure to any of the respiratory irritants. It also contributes to localized laryngeal inflammation.
According to a study, vocal cord dysfunction has been associated with multiple factors such as GERD, exercise, and nonspecific airways irritants.
Psychological Conditions
Various types of mental health conditions can serve as triggers for vocal cord dysfunction. Numerous individuals suffering from issues like anxiety disorder and clinical depression can feel suffocated or choked during a low phase. Episodes of post-traumatic stress disorder can add to your vocal cords’ poor movement. Psychogenic factors like emotional stress and depression have been recognized as potential triggers for paradoxical vocal cord dysfunction.
Vocal Cord Dysfunction Diagnosis
History & Physical Examination:
Diagnosing VCD is a challenging task for clinicians because of the overlapping symptoms with other respiratory conditions. However, doctors diagnose a patient presenting to the ER (with stridor, breathing difficulty, and hoarseness) by taking his history. Your healthcare professional will ask questions about your family history of asthma, and ask about your activity status and exposure to any environmental/respiratory irritants.
This is followed by a physical examination of your chest and lungs as the doctor listens to your chest sounds. However, a confirmed diagnosis is made based on the following diagnostic tests:
Laryngoscopy:
Flexible laryngoscopy is the most important diagnostic procedure to identify vocal cord dysfunction. It involves inserting a flexible tube containing a camera into your vocal cords to see their movement during inhalation. An ENT specialist (otolaryngologist) inserts the tube via your nose (or throat) and passes it to the larynx to visualize the vocal cords. After the camera is properly positioned, the doctor asks you to inhale. The adduction of the cords during inhalation makes the diagnosis easier.

A doctor is performing a laryngoscopy procedure in a patient suspected of vocal cord dysfunction.
Recent studies show that the use of functional laryngoscopy plays a crucial role in the diagnosis of VCD and aids in treatment planning.
Sometimes, doctors check the vocal cord response to a suspected trigger in a process known as a provocation test. The induction of an episode of cord dysfunction in response to smoke, ammonia, fumes, exercise, etc, validates the diagnosis of ILO.
Conventionally, laryngoscopy has been the main diagnostic tool for paradoxical vocal fold movement. However, experts now believe that computed tomography scans of the larynx have shown potential for a swift diagnosis.
Lung (Pulmonary) Function Tests:
Another test that reveals vital information regarding patients’ lung health is spirometry. Spirometry tests, done with a spirometer, measure the quantity of air inhaled and the quantity of air exhaled (plus the rate at which you exhale it). This test is done to rule out asthma and obstructive pulmonary disease. These tests do not diagnose VCD but help differentiate between VCD and conditions similar to it.
Differential Diagnosis:
There is a striking resemblance of VCD to other pulmonary conditions, which leads to frequent misdiagnosis. The differential diagnosis of ILO includes:
Vocal Cord Dysfunction Vs Asthma
The presentations of both disorders include throat tightness, breathing difficulty, and stridor. However, there are ample noticeable differences between the two. In VCD, the stridors and symptoms appear due to the adduction of the vocal cords. On the other hand, the cause of breathlessness in asthma is inflammation of the airways in response to a trigger (allergen, environmental toxin). Bronchodilators (in the form of inhalers) and corticosteroids curb the respiratory inflammation, which alleviates asthma symptoms. However, they have no response to vocal cord dysfunction. Moreover, the VCD involves your vocal cords, while asthma is a disease of the bronchial tubes.
Vocal Cord Dysfunction Vs Croup
Inducible laryngeal obstruction and croup have a common symptom of inspiratory stridor. VCD patients also have a higher-than-normal frequency of coughs. However, croup is characterized by a typical “barking cough,” which is absent in VCD patients. The underlying cause of croup is a viral infection that swells up the throat, while VCD is the outcome of poor vocal movement during inspiration. In some cases, asthma and vocal cord dysfunction can co-exist in a person, thereby making diagnosis even more difficult.
Vocal Cord Dysfunction Vs Laryngospasm
Laryngospasm is a more severe type of cord dysfunction in which there is a complete closure of the vocal cords, which leads to choking, stridor, and severe breathing difficulties.
Vocal Cord Dysfunction Treatment
The prime focus of all practitioners is to identify the patient-specific triggers and minimize their exposure. Treatment strategies vary according to the severity of the disease (mild, moderate, or severe). One study concluded that the use of respiratory training, low-dose amitriptyline, botulinum toxin injections, and inspiratory muscle strengthening (via training devices) shows promising results in resolving symptoms.
The most commonly employed strategies for VCD include:
Voice Therapy:
It is the most effective type of treatment option for inducible laryngeal obstruction. Taught by a speech-language pathologist, this treatment helps relax throat muscles, which helps you maintain optimal opening of the cords during episodes. Studies conclude that speech therapy is a safe and effective first-line treatment of vocal cord dysfunction. There are different subtypes of voice therapy. However, the most effective treatment for paradoxical vocal fold movement is the respiratory retraining therapy.
Respiratory Retraining Therapy
As the name indicates, this treatment modality retrains your respiratory muscles to improve essential activities like breathing, coughing, and swallowing. It comprises different breathing exercises that aid in the management of VCD symptoms. This therapy is often a part of music therapy that singers undergo to strengthen their respiratory muscles for enhanced performances.

A woman is doing diaphragmatic breathing (belly breathing to strengthen vocal cord muscles. This exercise reduces episodes of VCD.
Various vocal cord dysfunction exercises fall under respiratory retraining therapy that can help alleviate symptoms. Examples include pursed breathing and belly breathing (diaphragmatic breathing). These exercises are known to improve breathing during episodes of vocal cord-induced laboured breathing. Clinical literature suggests that long-term respiratory training for ILO has proven to be effective if the treatment is given at least once every 3 months.
Trigger Management:
In addition to strengthening the laryngeal muscles, doctors fix the underlying triggers that cause the paradoxical movements. Antacids and proton pump inhibitors for GERD, and antibiotics for upper respiratory tract infections, can help reduce the frequency of the episodes. However, there is no ultimate solution for the disease.
Final Word
Vocal cord dysfunction is a disorder in which your vocal cords (bands of muscle in the larynx) move to the midline (adduction) to impede the flow of air while you inhale. This produces inspiratory stridor, breathing trouble, throat tightness, and hoarseness. Patients also feel like having a lump in the throat and are often seen trying to clear out obstructions in the throat.
The exact cause of inducible laryngeal obstruction is unknown, but clinicians and patients have identified specific triggers that lead to the development of symptoms. The most common triggers include strenuous exercise, GERD, upper respiratory tract infection, and exposure to environmental irritants (like fumes, smoke, ammonia, chlorinated water in pools, etc.). Sometimes, psychological conditions like anxiety and depression can also contribute to paradoxical vocal fold movement.
Diagnosis of the condition is difficult and requires reaching a conclusive decision with the help of laryngoscopy. Healthcare practitioners often mistake VCD for croup and asthma. Thus, careful analysis of the cords is a must. Treatment involves managing the triggers (GERD medications and antibiotics, etc.) and strengthening the vocal cord muscles. Voice therapy, especially respiratory retraining therapy, uses breathing exercises to strengthen the vocal cords, which leads to better swallowing, coughing, and breathing. A speech-language pathologist also trains you how to manage your breath during an episode of VCD.
References
[1] Kenn, K., & Hess, M. M. (2008). Vocal cord dysfunction: an important differential diagnosis of bronchial asthma.Deutsches Ärzteblatt International,105(41), 699.Campainha, S., Ribeiro, C., Guimarães, M., & Lima, R. (2012). Vocal cord dysfunction: a frequently forgotten entity.Case Reports in Pulmonology,2012(1), 525493.
[2] Yap, G., Ruane, L. E., Hamza, K., Leahy, E., Avram, A., Baxter, M., … & Leong, P. (2023). Vocal cord dysfunction/inducible laryngeal obstruction cannot be diagnosed from symptoms. ERJ Open Research, 9(6), 00707-2023.
[3] Shires, C. B., & Dewan, K. (2024). Is there really a lump in my throat? The incidence and implications of vocal fold abnormalities in patients presenting with globus.Journal of Voice,38(6), 1419-1423.
[4] George, S., & Suresh, S. (2019). Vocal cord dysfunction: analysis of 27 cases and updated review of pathophysiology & management.International Archives of Otorhinolaryngology,23(02), 125-130.
[5] Leong, P., Vertigan, A. E., Hew, M., Baxter, M., Phyland, D., Hull, J. H., … & Bardin, P. G. (2023). Diagnosis of vocal cord dysfunction/inducible laryngeal obstruction: An International Delphi Consensus Study.Journal of Allergy and Clinical Immunology,152(4), 899-906.
[6] Leong, P., Vertigan, A. E., Hew, M., Baxter, M., Phyland, D., Hull, J. H., … & Bardin, P. G. (2023). Diagnosis of vocal cord dysfunction/inducible laryngeal obstruction: An International Delphi Consensus Study. Journal of Allergy and Clinical Immunology, 152(4), 899-906.
[7] Vertigan, A. E., Kapela, S. L., & Gibson, P. G. (2020). Chronic cough in vocal cord dysfunction: description of a clinical entity.Respiratory Medicine,168, 105990.
[8] Monoson, A., & Parsons, J. (2023). Exercise-Induced Bronchoconstriction and Vocal Cord Dysfunction. InEndurance Sports Medicine: A Clinical Guide(pp. 37-47). Cham: Springer International Publishing.
[9] Papamichael, M. M., & Katsardis, C. (2025). Exercise‐Induced Dyspnea: There is More to This Than Meets the Eye!—A Narrative Review.Journal of Paediatrics and Child Health.
[10] Papamichael, M. M., & Katsardis, C. (2025). Exercise‐Induced Dyspnea: There is More to This Than Meets the Eye!—A Narrative Review.Journal of Paediatrics and Child Health.
[11] Stoltz, L. P., Fajt, M. L., Petrov, A. A., & Traister, R. S. (2018). Vocal cord dysfunction: a review.Clinical Pulmonary Medicine,25(4), 125-130.
[12] Ambati, S. R., Kaslovsky, R., Evans, M. T., & Edge, W. (2023). Vocal cord dysfunction during the COVID-19 pandemic.Respiratory Care,68(4), 520-523.
[13] Fermin, P., & Tiene, S. (2021). A Case of Stridor.Proceedings of UCLA Health,24(1).
[14] Morris, M. J., & Christopher, K. L. (2010). Diagnostic criteria for the classification of vocal cord dysfunction.Chest,138(5), 1213-1223.
[15] McNeely, B. D., & Hu, A. (2023). Functional Disorders of the Larynx: Muscle Tension Dysphonia, Paradoxical Vocal Cord Dysfunction, and Globus Pharyngeus. InFunctional Illness of the Head and Neck(pp. 183-196). Cham: Springer International Publishing.
[16] Vertigan, A. E., Bone, S. L., & Gibson, P. G. (2022). The impact of functional laryngoscopy on the diagnosis of laryngeal hypersensitivity syndromes.The Journal of Allergy and Clinical Immunology: In Practice,10(2), 597-601.
[17] Leong, P., Gibson, P. G., Vertigan, A. E., Hew, M., McDonald, V. M., & Bardin, P. G. (2023). Vocal cord dysfunction/inducible laryngeal obstruction—2022 Melbourne Roundtable Report.Respirology,28(7), 615-626.
[18] Kumaresan, T., Thomas, M., Uppal, P. A., Setzen, S., Brar, S., Yalamanchili, A., … & Mortensen, M. (2023). Predictors of voice therapy efficacy in vocal cord dysfunction at a tertiary care center.American Journal of Otolaryngology,44(4), 103882.
[19] Mahoney, J., Hew, M., Vertigan, A., & Oates, J. (2022). Treatment effectiveness for vocal cord dysfunction in adults and adolescents: a systematic review.Clinical & Experimental Allergy,52(3), 387-404.
[20] Kumaresan, T., Thomas, M., Uppal, P. A., Setzen, S., Brar, S., Yalamanchili, A., … & Mortensen, M. (2023). Predictors of voice therapy efficacy in vocal cord dysfunction at a tertiary care center.American Journal of Otolaryngology,44(4), 103882.
[21] Nacci, A., Fattori, B., Segnini, G., Dallan, I., Panicucci, E., Rocchi, V., & Ursino, F. (2011). Respiratory retraining therapy in long-term treatment of paradoxical vocal fold dysfunction.Folia Phoniatrica et Logopaedica,63(3), 134-141.