
 is a rare type of white blood cell cancer that affects B-lymphocytes...){kind=link}

Waldenstrom Macroglobulinemia Symptoms Waldenstrom Macroglobulinemia (WM) is a rare type of white blood cell cancer that affects B-lymphocytes, a type of immune cell responsible for antibody production. The mutated cancer cells cause an increased production of IgM antibody in our blood that makes it thicker and reduces its flow to various organs throughout the body, leading to hyperviscosity syndrome (an increase in blood viscosity). The incidence of WM is higher in the older age group >65, in males, and in people with anemia (Hb ≤11.5 g/dL).
It is also known as lymphoplasmacytic lymphoma (LPL), because the cancer cells appear to be similar to both lymphocytes and plasma cells. It is, basically, a slow-growing type of non-Hodgkin lymphoma that is treatable if diagnosed earlier. Most patients (about 90–95%) have a mutation in the MYD88 (L265P) gene, considered the driver mutation of LPL. Around 30–40% of patients also have mutations in the CXCR4 gene, with more than 40 variants identified. The CXCR4 mutations can reduce the effectiveness of Bruton tyrosine kinase (BTK) inhibitors such as ibrutinib because of continuous activation of the chemokine receptor and development of alternate signaling pathways that lead to drug resistance.
Signs and Symptoms of Waldenstrom Macroglobinemia: Waldenstrom Macroglobulinemia Symptoms
The signs and symptoms of Waldenstrom Macroglobulinemia vary from patient to patient. Patients can be asymptomatic in earlier stages of the disease and the condition can remain stable for years under observation, but in later stages, severe complications arise that require immediate treatment.
• Anemia and Fatigue:
Anemia and the fatigue associated with it are the most common symptoms in patients with the disease and require medical intervention and therapy. There are two reasons for anemia in patients with WM. Firstly, there is bone marrow infiltration of cancer cells, leading to decreased formation of normal blood cells. Secondly and most importantly, there is an increase in the level of a peptide hormone known as hepcidin, which regulates the metabolism of iron in our body. There is reduced release of iron from its storage, leading to less blood cell formation, and hence anemia occurs in the patients.
• Bleeding disorders:
Bleeding occurs due to platelet dysfunction, alteration in coagulation factors, and fibrinogen, resulting from increased interaction with plasma IgM. We often observe nosebleeds, bleeding gums, and changes in vision due to bleeding in the retina.
• Lower Immunity:
Increased susceptibility to infection resulting from impaired B-cell function or T-cell function leads to decreased immunity against common illnesses like fever, flu, and other viral as well as bacterial infections.
• Gastrointestinal Problems:
Diarrhoea and insufficient nutrient absorption can occur due to gastrointestinal (GI) complications. In some people with WM, the buildup of IgM protein in the intestines can lead to problems such as diarrhea, poor absorption of vitamins, or gastrointestinal bleeding (seen as blood in stools or dark stools).
• Hyperviscosity syndrome:
Hyperviscosity syndrome is a life-threatening oncologic emergency that results from a high concentration of IgM proteins in the blood that presents classically as a triad of neurological deficits (headaches, vertigo, confusion), visual changes (blurred vision, retinal bleeding), and mucosal bleeding. These thickened proteins reduce blood flow and can lead to multiple organ complications, such as heart failure or stroke.
Patients with IgM levels below 3,000 mg/dL usually do not develop hyperviscosity, but treatment decisions depend on symptoms rather than IgM levels alone. Plasmapheresis is required immediately if hyperviscosity symptoms appear.
• Peripheral neuropathy:
The increase in neoplastic monoclonal IgM protein in neural cells leads to impaired sensory and motor functions of these cells as they attack the myelin-associated glycoprotein (MAG) on these cells.
• Bing Neel Syndrome:
BNS is a disorder caused by infiltration and accumulation of clonal lymphoplasmacytic cells (LPCs) in the central nervous system (CNS). In 1936, doctors Jens Bing and Axel Neel documented two individuals with neurological issues, hyperglobulinemia, and LPCs in their cerebrospinal fluid (CSF).
Patients frequently exhibit a wide range of neurological abnormalities, including balance difficulties, ataxia, sensory and motor impairments, headaches, and cognitive impairments. Imaging studies, investigations of CSF fluid, and biopsies are all viable methods to definitively establish a clinical diagnosis of BNS. The detection of IgH locus rearrangements and MYD88 L265P gene mutations may serve as effective diagnostic methods for BNS.
What are the Causes of Waldenstrom Macroglobulinemia?
Cancer happens when cells develop changes in their DNA. A cell’s DNA holds all the instructions that tell a cell what to do and when to die by its natural cycle. Changes in the DNA of white blood cells result in WM, but “why it occurs” is still a matter of debate. The following are some of the studies that state the cause as:
- The exact cause of the disease is unknown, but it is hypothesized that LPL/WM cells originate from B-cells, which are at the last stages of their maturation.
- Clonal B-cells (genetically identical abnormal cells) may appear in the blood of WM patients, although lymphocytosis (a high white blood cell count) is uncommon.
- The predominant source of abnormal cells in WM is thought to be IgM or IgM–IgD memory B-cells.
- Chromosomal abnormalities have been detected in the cells of WM patients, even in the absence of immunoglobulin heavy chain (IgH) translocations, which are commonly seen in other lymphoid cancers.
- Recent research also highlights the importance of the bone marrow tumor microenvironment in WM progression. The bone marrow contains stromal cells, mast cells, endothelial cells, and immune cells that produce cytokines and growth factors supporting malignant B-cell survival and proliferation

Schematic representation of some of the cells present in the WM tumor microenvironment. Image adapted from Boutilier AJ, Huang L, & Elsawa SF.Waldenström Macroglobulinemia: Mechanisms of Disease Progression and Current Therapies.Int J Mol Sci.2021;23(19):11145. available viaMDPIunder license CC BY 4.0
How to Diagnose Waldenstrom Macroglobulinemia?
WM is defined by the presence of lymphoplasmacytic infiltration of bone marrow with an associated monoclonal IgM protein, usually when ≥10% of bone marrow cells are lymphoplasmacytic. If infiltration is lower, the condition is classified as IgM MGUS (monoclonal gammopathy of undetermined significance) or smoldering WM.
The 2017 World Health Organization classification of tumors of hematopoietic and lymphoid tissues had established four diagnostic criteria for Waldenstrom macroglobulinemia, including:
- Presence of IgM monoclonal gammopathy
- Infiltration of bone marrow by small lymphocytes showing plasmacytoid or plasma cell differentiation
- Bone marrow infiltration showing an intertrabecular pattern
- Immunophenotype supportive of Waldenstrom macroglobulinemia that including surface IgM+, CD19+, CD20+, CD22+, CD25+, CD27+, FMC7+, and negative for CD10 and CD23
The diagnosis usually begins with the history and physical examination. The steps are listed below:
1. History and Examination:
Taking a detailed history of the patient and examination for various symptoms is crucial to developing a diagnosis. Patients may present with fatigue, weakness, mucosal bleeding, neuropathy, or signs of hyperviscosity. Look for pallor, organomegaly (especially splenomegaly), lymphadenopathy, or signs of bleeding.
2. Laboratory Tests:
Blood Tests:
A complete blood count (CBC) reveals a decrease in both red (anemia) and white blood cell counts (Leukopenia), a low platelet count (Thrombocytopenia). Other findings may include elevated serum viscosity, raised beta-2 microglobulin, and increased uric acid levels. Serum protein electrophoresis (SPEP) typically reveals an IgM monoclonal spike.
Urine Tests:
Urinalysis may reveal proteinuria due to the presence of light chains (Bence-Jones protein), although this is less common than in multiple myeloma..
3. Biopsy:
Histopathological examination, bone marrow aspiration, and flow cytometry help confirm lymphoplasmacytic infiltration and define the immunophenotype.
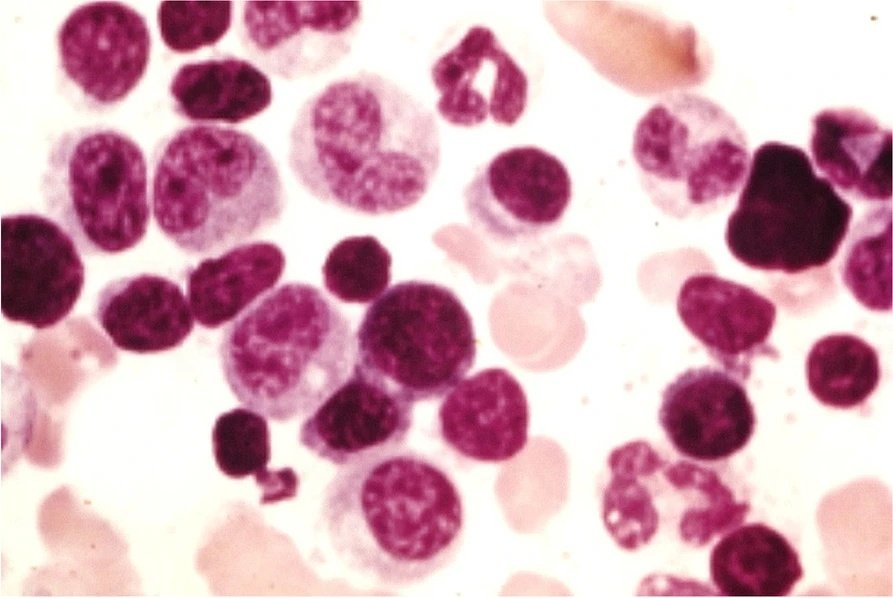
Bone marrow smear showing lymphoplasmacytic cells in a patient with Waldenstrom Macroglobulinemia. These cells display features of both small lymphocytes and plasma cells, characteristic of the disease.. Image courtesy: Awad, A. K., Elbadawy, M. A., Boury, M., Rivera, A., Motawea, K., Shah, J., Parnia, S., & Varney, J. (2022). Simple headache revealed a rare lymphoma: Waldenstrom macroglobulinemia with unique markers: A case report and review of the literature.Journal of the Egyptian National Cancer Institute,34(1), 1-4. available viaSpringerOpenUnder license CC BY 4.0
4. Imaging and Other Investigations:
A chest/abdominal CT or a PET Scan is an important step in making a diagnosis of WM. For Bing-Neel Syndrome specifically, MRI brain and spine, cerebrospinal fluid (CSF) analysis (cytology, flow cytometry, protein, and glucose measurement) is essential. For Hyperviscosity syndrome specifically, retinal examination (if IgM >3.0 g/dl), scan for splenomegaly, and lymph node assessment for lymphadenopathy help in making the diagnosis.
Classification of WM and related disorders
Waldenstrom Macroglobulinemia can be classified into four groups. The features of each group are summarized in the following table.
Table: Classification of Waldenström’s macroglobulinemia and related disorders.
| IgM monoclonal protein | Bone marrow infiltration | Symptoms attributable to IgM | Symptoms due to tumor infiltration | |
|---|---|---|---|---|
| Symptomatic WM | Positive | Positive | Positive | Positive |
| Asymptomatic WM | Positive | Positive | Negative | Negative |
| IgM-related disorders | Positive | Negative | Positive | Negative |
| IgM-MGUS | Positive | Negative | Negative | Negative |
Differential Diagnosis of WM
WM must be differentiated from several other lymphoproliferative and plasma cell disorders. For that purpose, a bone marrow biopsy is a crucial test. The following are the key differentiating factors of some diseases from WM:
| Condition | Immunoglobulin Type | Bone Marrow Findings | Key Clinical Features | Distinguishing Features from WM |
|---|
| Multiple Myeloma (MM) | Usually IgG or IgA (rarely IgM) | Plasma cell proliferation | Bone pain, lytic lesions,hypercalcemia, renal failure | CRAB features (hyperCalcemia, Renal failure, Anemia, Bone lesions) common; IgM rare |
|---|
| Monoclonal Gammopathy of Undetermined Significance (MGUS) | Often IgG, sometimes IgM | <10% plasma or lymphoplasmacytic cells | Asymptomatic | No organ damage, M-protein <3 g/dL, no anemia or hyperviscosity |
|---|
| Chronic Lymphocytic Leukemia (CLL) | Often IgM or IgG (monoclonal) | Mature small lymphocytes | Lymphadenopathy, hepatosplenomegaly, lymphocytosis | Peripheral lymphocytosis, CD5+, CD23+, less hyperviscosity |
|---|
| Marginal Zone Lymphoma (MZL) | Variable (often IgM) | Small B-cell infiltrate | Extranodal involvement (esp. spleen, MALT) | MYD88 mutation uncommon |
|---|
| Splenic Marginal Zone Lymphoma (SMZL) | Usually IgM | Intrasinusoidal lymphoid infiltrate | Splenomegaly, cytopenias | Prominent splenomegaly, few plasma cells |
|---|
| Heavy Chain Disease (α-, γ-, or μ-chain) | Heavy chain only (no light chain) | Variable lymphoplasmacytic infiltrate | Malabsorption (α-chain), lymphadenopathy (γ-chain) | Absence of intact immunoglobulin; only heavy chain fragments |
|---|
| Cold Agglutinin Disease (CAD) | IgM (autoantibody) | Variable, no clonal infiltration | Hemolytic anemia, acrocyanosis | Autoimmune hemolysis; no monoclonal neoplasm |
|---|
| Lymphoplasmacytic Lymphoma (LPL) | Usually IgM | Lymphoplasmacytic infiltrate | Hyperviscosity, anemia, neuropathy | WM is a subset of LPL with IgM monoclonal gammopathy |
|---|
Prognostic Scoring Systems of WM
Waldenstrom macroglobulinemia (WM) doesn’t use a standard cancer staging system. Instead, doctors use something called a prognostic score to help understand how the disease might behave and how it may affect a person’s lifespan.
The three scoring systems of WM are as follows:
1. International Prognostic Scoring System for Waldenstrom Macroglobulinemia (IPSSWM):
The most common tool is called the International Prognostic Scoring System for Waldenstrom Macroglobulinemia (IPSSWM). It’s used for people with WM who need treatment.
This score is based on five things:
- Age> 65 years
- Hemoglobin level (a measure of red blood cells) ≤11.5 g/dL
- Platelet count ≤100 × 10⁹/L
- Beta-2 microglobulin level (a protein that can show how active the disease is) >3 mg/L
- Monoclonal IgM level in your blood (a type of antibody made by WM cells) >7 g/dL
2. Revised (r) IPSS-WM:
The International Prognostic Scoring System for WM (IPSS-WM) emerged from a collaborative effort to stage patients requiring treatment into three groups based on five parameters: age, platelet count, hemoglobin, beta-2 microglobulin (β2M), and IgM level. The IPSS-WM did not assess the issue of non–WM-related deaths. The recently proposed, revised (r) IPSS-WM, based on age, lactate dehydrogenase (LDH), albumin, and β2M, addressed some of the deficiencies. The score criterion is as follows:
- Age: 66-75 years
- Beta-2 microglobulin >4mg/dL
- Serum albumin <3.5 g/dL
- Lactate dehydrogenase(LDH) >250 IU/L (upper limit of normal <225 IU/L)
3. MSS-WM (Modified Staging System):
Incorporates molecular markers such as MYD88 L265P mutation, which is now routinely tested.
- Age 66–75 years = 1 point; >75 years = 2 points
- Serum albumin <3.5 g/dL = 1 point
- Elevated LDH = 2 points
Patients are classified into risk groups based on their total score:
- Low-risk: 0–1 points
- Intermediate-risk: 2–3 points
- High-risk: ≥4 points
Prognosis of WM
WM is a chronic and indolent illness, and asymptomatic patients generally have better survival outcomes. In early stages, it is treatable and manageable, although not curable. Long-term studies (5–10 years) show that advanced age (>65 years), male gender, and hemoglobin levels below 11.5 g/dL are associated with a poorer prognosis. According to recent research, the median survival of symptomatic patients is 8–10 years. Asymptomatic patients should not receive treatment immediately but should be regularly monitored.
Waldenstrom Macroglobulinemia Treatment
The treatment of Waldenstrom Macroglobulinemia is a step-wise approach in relation to the severity of the disease. The disease is treatable if diagnosed at earlier stages. Treatment choice should take into account specific goals of therapy, necessity of rapid disease control and risk of treatment-related complications. Following is the general treatment plan of Waldenstrom Macroglobulinemia:
Patients without symptoms:
Patients with elevated IgM protein but no symptoms might not need the treatment right away. Instead, doctors can take the blood samples every few months to monitor the condition. They call it watchful waiting and during this period, Waldenstrom Macroglobulinemia is observed with care without therapy.
Symptomatic Patients (mild condition):
Patients with mild hematological compromise, IgM-related neuropathy, or cold agglutinin hemolysis are treated with standard doses of rituximab alone without maintenance therapy.
Symptomatic Patients (severe condition):
Patients with severe symptoms like severe anemia, hyperviscosity syndrome, or organ involvement should receive combination therapy. Common regimens include:
- DRC (dexamethasone, rituximab, and cyclophosphamide)
- Bendamustine-rituximab (BR)
- BTK inhibitors such as ibrutinib or zanubrutinib
- In cases of hyperviscosity, treatment should begin with plasmapheresis, a procedure that removes excess IgM and other harmful proteins from the blood. This is followed by drug therapy (BTK inhibitors or DRC regimen).
- Stem-cell transplant can also be considered if a relapse occurs.
Waldenstrom Macroglobulinemia vs Multiple Myeloma
Waldenstrom Macroglobulinemia and Multiple Myeloma are two different diseases with the common finding of IgM monoclonal gammopathy. However, they differ in pathogenesis, cell origin, and clinical presentation.
| Feature | Waldenstrom Macroglobulinemia (WM) | Multiple Myeloma(MM) |
|---|---|---|
| Cell of Origin | B lymphocytes (lymphoplasmacytic cells) | Mature plasma cells |
| Main Monoclonal Protein | IgM | IgG, IgA, or free light chains |
| Plasma Cell Percentage in Bone Marrow | Usually less than 10% | Typically greater than 10% |
| Genetic Abnormality | MYD88 L265P mutation present in ~90% of cases | MYD88 mutation absent |
| Bone Involvement | Rare; lytic lesions uncommon | Common; lytic bone lesions typical |
| Lymphoid Organ Involvement | Splenomegaly and lymphadenopathy common | Rare |
| Bone Marrow Involvement | Mild to moderate infiltration | Extensive infiltration |
| Serum Viscosity | Frequently increased due to excess IgM | Usually normal |
| Hyperviscosity Syndrome | Common | Rare |
| Renal Dysfunction | Uncommon | Common due to light chain deposition |
| Common Symptoms | Fatigue, anemia, mucosal bleeding, vision problems, neuropathy | Bone pain, fractures, hypercalcemia, renal failure |
| Prognosis | Indolent and chronic; may not require immediate treatment | More aggressive; needs early treatment |
| First-Line Treatment | Watchful waiting (if asymptomatic), rituximab-based regimens, BTK inhibitors, plasmapheresis for hyperviscosity | Chemotherapy, immunomodulatory drugs, proteasome inhibitors, corticosteroids |
| Stem Cell Transplant | Considered in relapsed or refractory cases | Common in eligible patients for consolidation therapy |
Conclusion:
In short, Waldenstrom Macroglobulinemia is a rare hematological cancer that develops more commonly in older age groups with Hb levels below 10gm/dL. It develops due to mutations in DNA responsible for IgM antibody production, which leads to the formation of excessive monoclonal IgM protein that infiltrates through various body organs, leading to severe complications. It can be asymptomatic, which can resolve by careful monitoring of the suffering patients or can be symptomatic, which requires a comprehensive and step-wise treatment approach according to the severity of the condition.
References
[1] Bibas, M., Sarosiek, S., & Castillo, J. J. (2024). Waldenström macroglobulinemia – A state-of-the-art review: Part 1: Epidemiology, pathogenesis, clinicopathologic characteristics, differential diagnosis, risk stratification, and clinical problems.Mediterranean Journal of Hematology and Infectious Diseases, 16(1), e2024061.
[2] Morel P, Duhamel A, Gobbi P, et al: International Prognostic Scoring System for Waldenstrom macroglobulinemia.Blood113:4163-4170, 2009
[3] García-Sanz R, J. C. (2021). Time to move to the single-cell level: applications of single-cell multi-omics to hematological malignancies and Waldenström’s macroglobulinemia particularly heterogeneous lymphoma. Cancers(Basel).
[4] Banwait R, A. Y.-P. (2015). Extramedullary Waldenström macroglobulinemia. Am J Hematol.
[5] Minnema MC, K. E. (2017). . Guideline for the Diagnosis, Treatment and Response Criteria for Bing-Neel Syndrome. Haematologica., 43-51.
[6] Oishi N, I. T. (2020). Composite monoclonal B-cell lymphocytosis and MYD88 L265P-positive lymphoplasmacytic lymphoma in a patient with IgM light chain amyloidosis:. Pathol Int. .
[7] Smith BR, R. N. (1983). In Waldenström’s macroglobulinemia, the quantity of detectable circulating monoclonal B lymphocytes correlates with clinical course. Blood.
[8] Wagner SD, M. V. (1994). Similar patterns of V kappa gene usage but different degrees of somatic mutation in hairy cell leukemia, prolymphocytic leukemia, Waldenström’s macroglobulinemia, and myeloma. Blood.
[9] Swerdlow SH, Campo E, Pileri SA, Harris NL, Stein H, Siebert R, Advani R, Ghielmini M, Salles GA, Zelenetz AD, Jaffe ES. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016 May 19;127(20):2375-90.
[10] Dogliotti, I., Jiménez, C., Varettoni, M.et al.Diagnostics in Waldenström’s macroglobulinemia: a consensus statement of the European Consortium for Waldenström’s Macroglobulinemia.Leukemia37, 388–395 (2023). https://doi.org/10.1038/s41375-022-01762-3
[11] Morel P, Duhamel A, Gobbi P, et al: International Prognostic Scoring System for Waldenstrom macroglobulinemia. Blood 113:4163-4170, 2009.
[12] Castillo JJ, Olszewski AJ, Kanan S, et al: Overall survival and competing risks of death in patients with Waldenström macroglobulinemia: An analysis of the surveillance, epidemiology and end results database. Br J Haematol 169:81-89, 2015.
[13] Zanwar, S., Abeykoon, J. P., Durot, E., Tomowiak, C., Kanagaratnam, L., Kanoria, S., … Castillo, J. J. (2024).Modified Staging System for Waldenström Macroglobulinemia (MSS-WM): A simple, externally validated prognostic model for symptomatic WM.Journal of Clinical Oncology
[14] Gertz, M. A. (2021). American Journal of Hematology, 96(3), 258–269.
[15] Ansell, S. M. (2010). Stem cell transplant. Mayo Clinic Proceedings, 824-833.