
{kind=link}

One of the most common skin problems worldwide, probably even more thanacne, is having an uneven skin tone. It’s not a medical emergency in any way, but it has a huge impact on a person’s confidence and quality of life. And it affects people of all ages and skin types, though some more drastically.
The term uneven skin tone can point to several conditions: hyperpigmentation, dark spots, redness, dullness, or blotchiness. Sun exposure is the single most common aggravating factor. Whatever the cause, it is largely manageable if treated right and with consistency. The problem is that a lot of people don’t try to pinpoint the cause and end up using the wrong products for a while before going to a dermatologist.
What is Uneven Skin Tone?
Uneven skin tone is an umbrella term that refers to the irregular distribution of pigment in an area of the skin. This pigment is melanin, and it pretty much single-handedly determines the skin’s colour. When the production of this melanin becomes irregular, it results in patches that are darker, lighter, redder, or duller than the surrounding skin.
It can be triggered by UV, hormones, inflammation, or injury, based on the type:
- Hyperpigmentation, where excess melanin causes dark patches
- Post-inflammatory hyperpigmentation, left behind after acne, eczema, or skin trauma, anything that causes the skin to become inflamed
- Melasma, hormonally driven
- Sun spots or age spots from cumulative UV damage because of prolonged exposure to the sun
- Erythema (redness) from rosacea or chronic inflammation
- Hypopigmentation, which is a loss of pigment following a burn or after some inflammatory conditions
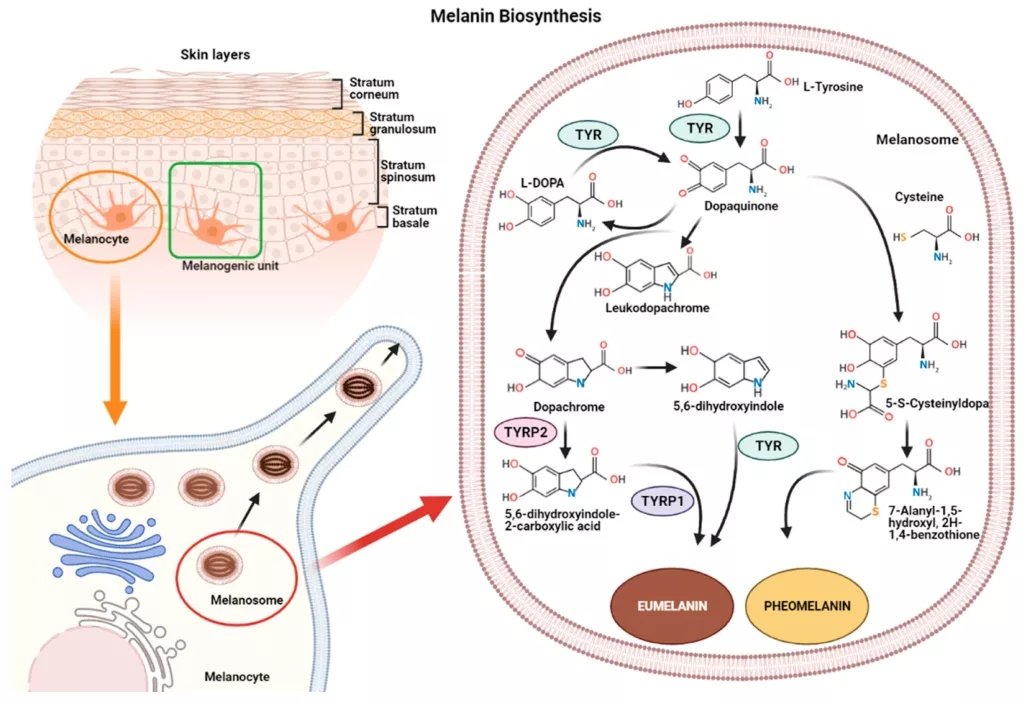
Melanin biosynthesisinvolves the tyrosinase enzyme (TYR) that converts amino acids into the two types of melanin pigment: eumelanin and pheomelanin. (Image Courtesy: Hushcha, Y., Blo, I., Oton-Gonzalez, L., Mauro, G. D., Martini, F., Tognon, M., & Mattei, M. D. (2021). microRNAs in the Regulation of Melanogenesis. International Journal of Molecular Sciences, 22(11), 6104. Available fromMDPIand licensed under CC by 4.0)
How Does Uneven Skin Tone Develop?
People think melanin causes hyperpigmentation. That is not true; melanin is a naturally occurring pigment in the skin, produced inside melanocytes through a process called melanogenesis. For this process, the main enzyme is tyrosinase, which is why most brightening ingredients work by inhibiting tyrosinase.
Two types of melanin are produced: eumelanin (brown/black) and pheomelanin (red/yellow). The ratio between these two determines a person’s skin and hair color, undertones, etc. So, everyone has both, just in different proportions.
When this melanin is produced, it gets packaged into organelles (melanosomes) inside the melanocytes, and then transferred to surrounding keratinocytes via dendrites (finger-like extensions of the melanocyte). One melanocyte supplies approximately 36 surrounding keratinocytes; this unit is sometimes called the epidermal melanocyte unit.
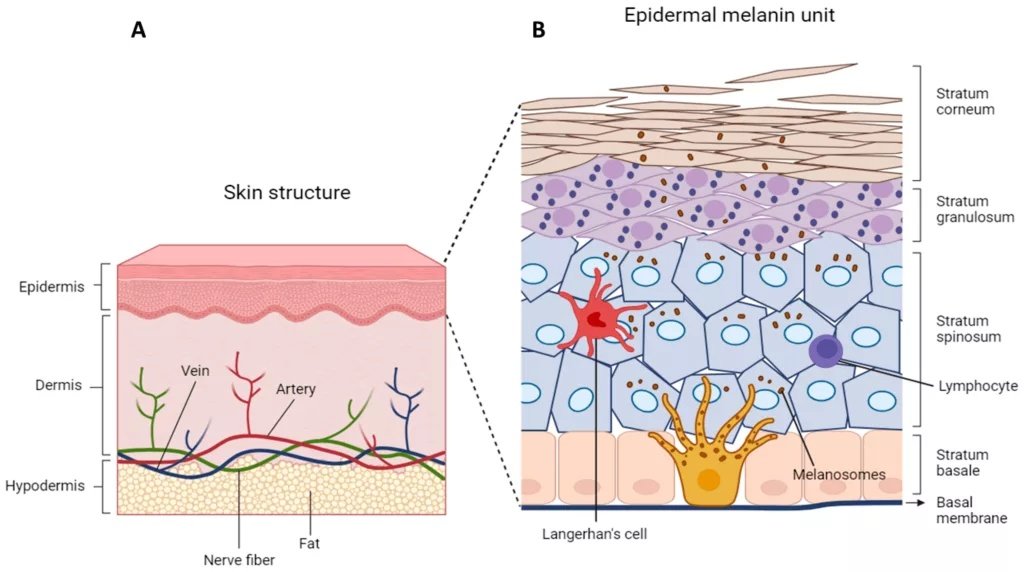
Anatomy of the Skin and the Epidermal-Melanin Unit:(A) A cross-section of the three primary layers: the epidermis, dermis, and hypodermis. (B) A close-up of the Epidermal-Melanin Unit, showing a dendritic melanocyte in the basal layer. This specialized cell synthesizes melanin within melanosomes and distributes it to approximately 36 surrounding keratinocytes, where it forms a protective pigment cap over the cell nuclei. (Image Courtesy: Marrapodi, R., & Bellei, B. (2024). The Keratinocyte in the Picture Cutaneous Melanoma Microenvironment. Cancers, 16(5), 913. Available fromMDPIand licensed under CC by 4.0)
In normal skin, this transfer is even and regulated, so the result is a uniform tone. The melanocyte does not keep producing melanin passively; it does so actively, regulated in response to signals from keratinocytes, UV, and hormones.
When this system is disrupted by one of the triggers, melanocytes end up overproducing or misdistributing the melanin, and the result is uneven tone visible at the surface.
In darker skin types, melanosomes are larger and distributed more broadly within the keratinocytes. This is the principle why deeper skin tones tan rather than burn, and more importantly, why their inflammatory pigmentation response is stronger. This makes PIH both more common and harder to treat.
What Causes Uneven Skin Tone?
There are several well-known facts that trigger the melanocytes, some of which are:
- UV radiation is the single most common cause, and it’s something everyone gets exposed to every day. UV stimulates melanocytes to overproduce melanin in exposed areas, and with sun damage over a long time, it drives dark spots and uneven tone.
- Hormonal changes can cause an uneven skin tone directly or indirectly by causing inflammation (e.g., hormonal acne). Oestrogen and progesterone directly stimulate melanocyte activity; this is why melasma appears or worsens in pregnancy and with oral contraceptive use.
- Inflammation, like acne, eczema, cuts, burns, waxing, or any trauma, triggers melanin release as part of the healing process. Even after the original injury is long gone, it might leave a dark mark.
- It’s a natural, unpreventable process, but with ageing, cell turnover slows down; this means dead skin cells are left to accumulate on the surface, and long-term UV damage turns into visible unevenness.

Primary Triggers of Melanin Overproduction. (1) UV Radiation stimulates melanocytes directly, (2) Hormonal Fluctuations (like those in pregnancy or from oral contraceptives) drive melasma, (3) Post-Inflammatory Hyperpigmentation (PIH) results from skin trauma like acne or burns, and (4) Ageing slows the natural shedding of pigmented cells.
- Genetics, of course, can be the biggest factor for some people. The baseline melanocyte activity and skin type are inherited. And then darker skin types have more reactive melanocytes and are more prone to PIH.
- Certain medications, antibiotics, antimalarials, and chemotherapy agents can also cause hyperpigmentation as a side effect.
- There are certain skin conditions that are often chronic (like rosacea, eczema, and psoriasis) and cause persistent inflammation, which, over time, drives post-inflammatory pigmentation.
- Poorly controlled systemic inflammation may also manifest in the skin by causing melanocytes to overproduce.
Lifestyle Factors
- Then there are some internal factors as well. Nutritional deficiencies like Vitamin B12 and folate deficiency (in some cases) can cause hyperpigmentation, particularly on the hands, face, and mucous membranes. Vitamin B12 deficiency is more common in vegans and people using metformin. Besides nutritional deficiencies, no particular food is proven to cause or fix hyperpigmentation in otherwise healthy people.
- In other lifestyle factors, chronic stress elevates cortisol, which causes inflammation and impairs the skin barrier function. Poor sleep also slows down skin repair. Neither of these causes hyperpigmentation directly, but both worsen the skin’s condition and make it vulnerable to damage from the outside.
Uneven Skin Tone on The Face
The face is almost always more affected by uneven skin tone or hyperpigmentation than other parts of the body. One reason for this is understandable enough: it receives the highest UV exposure. The second reason, however, is that facial skin is thinner and more reactive, making it more susceptible to PIH.
Hyperpigmentation on the face follows some common, predictable patterns:
- Cheeks and nose (sun damage, rosacea redness)
- Upper lip and forehead (melasma)
- Around the mouth and along the jaw (hormonal, PIH from shaving or waxing)
- Under the eyes (vascular or pigmentary)
How to Fix Uneven Skin Tone?
Because of the variety of causes, there is no single fix; the treatment of choice depends on pinpointing the cause and depth of pigmentation. For example, superficial (epidermal) pigmentation responds well to topical treatments and chemical exfoliation. Deeper (dermal) pigmentation, such as long-standing melasma, is harder to treat and even harder to prevent from recurring.
Topical Treatments
In general, clinicians prescribe one or a combination of topical ingredients with the strongest evidence against hyperpigmentation. It’s important to remember, however, that topical treatments require consistency; usually, 8-12 weeks of consistent use is required before results are visible.
They can be classified according to their underlying mechanisms:
Tyrosinase inhibitors4Zolghadri, S., Bahrami, A., Hassan Khan, M. T., Munoz-Munoz, J., Garcia-Molina, F., Garcia-Canovas, F., & Saboury, A. A. (2019). A comprehensive review on tyrosinase inhibitors. Journal of enzyme inhibition and medicinal chemistry, 34(1), 279–309.:
- Hydroquinone (the gold standard). Its use has to be consistent and controlled; long-term use has several side effects.
- Azelaic acid (anti-inflammatory) is particularly useful for PIH and rosacea-related redness
- Alpha arbutin is gentler than hydroquinone, so its administration doesn’t need to be monitored as hard
- Kojic acid
- Vitamin C
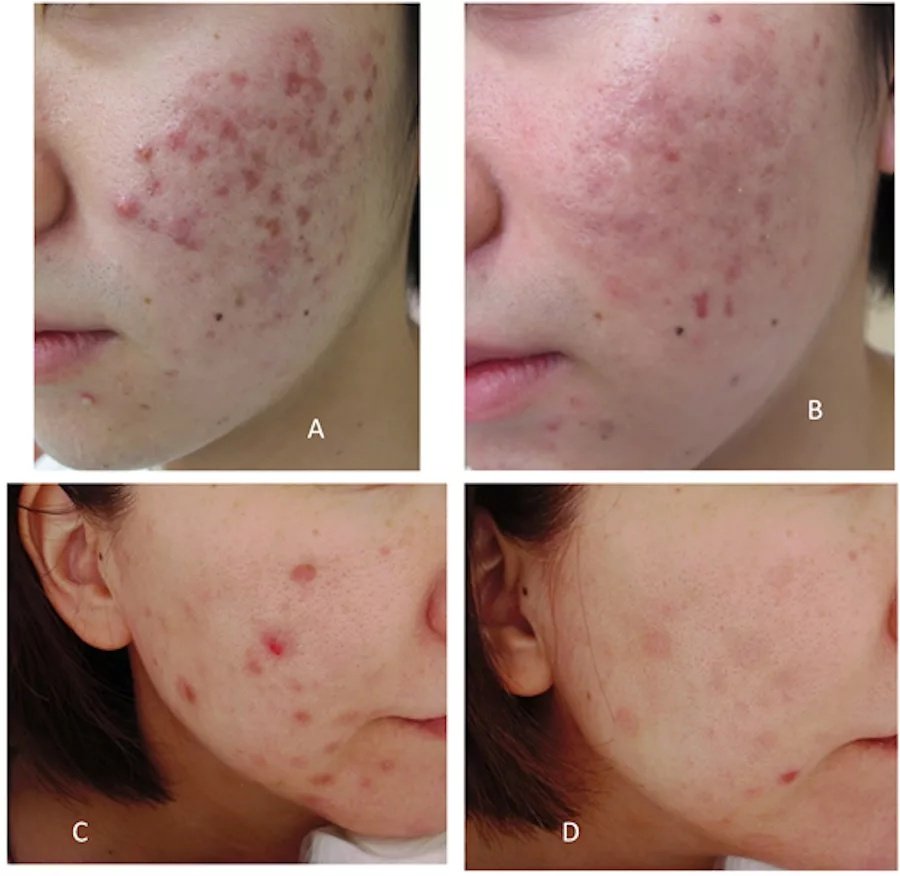
Reversing Inflammatory Damage. Clinical before-and-after showing the impact of a 3-month Vitamin C regimen on complex pigmentation. Note the improvement in both brown melanin patches (PIH) and persistent vascular redness (PIE), demonstrating Vitamin C’s dual role as an antioxidant and tyrosinase inhibitor. (Image Courtesy: Kurokawa, I.,Watanabe, M., and Hayashibe, K. (2020). Effect of a Cosmetic Use with 2% Isos-tearyl-L-Ascorbic Acid Gel for Postinflammatory Hyperpigmentation and Postinflammatory Erythema in Acne Vulgaris. Journal of Cosmetics, Dermatological Sciences and Applications, 10, 28-32. Available fromSCIRPand licensed under CC by 4.0)
Cell Turnover Accelerators:
- Retinoids (retinol, tretinoin) are recommended to slow down signs of aging because they accelerate cell turnover and push pigmented cells to the surface faster; they also inhibit tyrosinase.
- AHAs (glycolic acid, lactic acid) are chemical exfoliants that speed up cell turnover and improve overall radiance and texture
Transfer Blockers:
- Niacinamide inhibits melanosome transfer, not the synthesis. It also reduces redness and strengthens the skin barrier
Professional Treatments:
Other than these options, there are professional treatments available as well, offered in dermatology and aesthetic clinics:
- Chemical peels (glycolic, TCA, Jessner’s) offer deeper exfoliation and are known to be effective for hyperpigmentation
- Laser treatments like IPL, fractional lasers target melanin directly, but they must be used cautiously in darker skin types due to the risk of PIH
- Microneedling is another effective option that stimulates collagen and helps with skin texture and mild pigmentation
Sunscreen for Uneven Skin Tone:
The foundation of treating and preventing uneven skin tone is sunscreen. Once considered a gimmick, it is now a must-include in skincare for everyone, regardless of where they live. The recommended strength is SPF 50 broad-spectrum daily.Without using sunscreen, topical treatments are undermined because UV continues to stimulate the melanocytes. Even among sunscreens, tinted ones with iron oxides are particularly prescribed for melasma since they also protect against visible light.

The Protective Mechanism of Broad-Spectrum Sunscreen.(A) Without protection, UV radiation penetrates the epidermis, triggering melanocytes to overproduce and distribute melanin, resulting in visible dark spots.(B) Applying sunscreen creates a functional barrier on the skin’s surface.(C) Broad-spectrum SPF 50 filters both UVA and UVB rays, preventing the signaling cascade that leads to sun-induced damage and allowing existing hyperpigmentation to heal without further stimulation. (Image Courtesy: Fonseca, M., Rehman, M., Soares, R., & Fonte, P. (2023). The Impact of Flavonoid-Loaded Nanoparticles in the UV Protection and Safety Profile of Topical Sunscreens. Biomolecules, 13(3), 493. Available fromMDPIand licensed under CC by 4.0)
Conclusion
An uneven skin tone is understandably troubling for most people. With skincare advice so rampant, most people start with OTC products, which is reasonable, but they need to be the right products for the right cause, used consistently for at least 8-12 weeks before judging results. It’s time to get an in-depth consultation if:
- OTC products don’t show results after 3 months of consistent use; you might not be treating the right cause
- Melasma is worsening, a prescription triple combination cream (hydroquinone + tretinoin + steroids) may be needed, and cannot be self-administered safely
- Pigmentation appeared suddenly and with no clear trigger, which might indicate a systemic cause
- An existing dark spot that changes rapidly, it warrants assessment to rule out melanoma
For in-clinic procedures, always consult a qualified dermatologist, not an aesthetician without medical supervision, especially for darker skin types where procedure-induced PIH is a real risk.
References
[1] Yadav, G., Sauder, M., Siddha, S., Zeinab, R., Barakat, M., & Joseph, M. (2026). A Review of Post-Inflammatory Pigmentation Changes: Pathophysiology, Diagnosis and Treatment. Journal of cutaneous medicine and surgery, 12034754261427395. Advance online publication.
[2] Jangda, A., Voloshyna, D., Ramesh, K., Bseiso, A., Shaik, T. A., Al Barznji, S., Usama, M., Saleem, F., & Ghaffari, M. A. Z. (2022). Hyperpigmentation as a Primary Symptom of Vitamin B12 Deficiency: A Case Report. Cureus, 14(9), e29008.
[3] Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma.J Am Acad Dermatol.2006;54(5 Suppl 2):S272–81.
[4] Zolghadri, S., Bahrami, A., Hassan Khan, M. T., Munoz-Munoz, J., Garcia-Molina, F., Garcia-Canovas, F., & Saboury, A. A. (2019). A comprehensive review on tyrosinase inhibitors. Journal of enzyme inhibition and medicinal chemistry, 34(1), 279–309.
[5] Mukherjee, S., Date, A., Patravale, V., Korting, H. C., Roeder, A., & Weindl, G. (2006). Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clinical interventions in aging, 1(4), 327–348.
[6] Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma.J Am Acad Dermatol.2006;54(5 Suppl 2):S272–81.
[7] Wongdama, S., Yenyuwadee, S., Li, J. B., Saokaew, S., Kanchanasurakit, S., & Manuskiatti, W. (2026). Interventions to Prevent Postinflammatory Hyperpigmentation After Laser and Energy-Based Device Treatments: A Systematic Review and Network Meta-Analysis. Lasers in surgery and medicine, 58(3), 157–168.
[8] Morriss, S., & Scardamaglia, L. (2025). Sun protection: a practical guide for health professionals. Australian prescriber, 48(5), 173–178.