
{kind=link}

Melasma treatment Melasma, also called chloasma, common acquired hyperpigmentation disorder influenced by genetic predisposition, ultraviolet (UV) radiation, visible light, and hormonal factors caused by an excess of melanin in areas exposed to light. It causes light-to-dark-brown symmetrical, irregular, well-defined macules and patches on the skin. Melasma appears most commonly in sun-exposed areas like the face (upper lip, nose, cheeks, chin, and forehead) and in the cervical region. It may appear less on the forearms and sternal region. Melasma is sometimes referred to as the “mask of pregnancy” if it develops during pregnancy. The pigmentation normally deepens and lightens over time, usually becomes more severe in the summer, and improves in the winter.
The etiology of the disease multifactorial and not completely understood. Some predisposing factors include sun exposure, hormones, pregnancy, use of phototoxic drugs, genetic factors, use of cosmetics, and anticonvulsant drugs.

Freckles, dark spots, hyperpigmentation (melasma or chloasma)
The most common pigmentary condition among Asians is melasma, and it predominantly affects women, especially during their reproductive years. According to the American Academy of Dermatology, approximately 5 to 6 million women in the United States develop melasma. However, around 10% of cases also occur in men.
It is more common in women, especially those who have a darker skin tone and those who live in regions with intense sun exposure. It is a chronic and relapsing disorder that may require ongoing treatment. However, this disease is medically harmless but cosmetically significant. Chloasma can have a significant negative impact on many women. Psychological distress and tremendous emotional stress are chronic emotions caused by melasma.
Types of Melasma: Melasma treatment
Melasma has been classified into four major types based on the visible light and Wood’s light examination, although this method has limitations, and mixed-type melasma is now considered the most common form.
- Epidermal melasma
- Dermal melasma
- Mixed melasma
- Indeterminant or inapparent melasma
Epidermal Melasma
This form of melasma mostly affects the epidermis (outer layer of skin). It presents as well-defined brown macules that are clearly visible on the skin surface. The pigmentation is usually light to medium brown and becomes more pronounced under Wood’s lamp examination. Under histopathological examination, more melanin appears to be in the basal and suprabasal epidermal layers, and little melanin is in the papillary dermis. Epidermal melasma is more responsive to topical depigmenting, chemical peels, and strict photoprotection than dermal or mixed melasma due to the topical location of melanin.
Dermal melasma
This typically appears blue-gray or ash-colored on visual examination. On the Wood’s lamp assessment, the pigmentation does not show enhancement, and the borders appear poorly defined. Histologically, there is less noticeable epidermal hyperpigmentation, superficial and deep dermal melanophages, and vacuolar degeneration of basal cells and the sub-basement membrane zone.
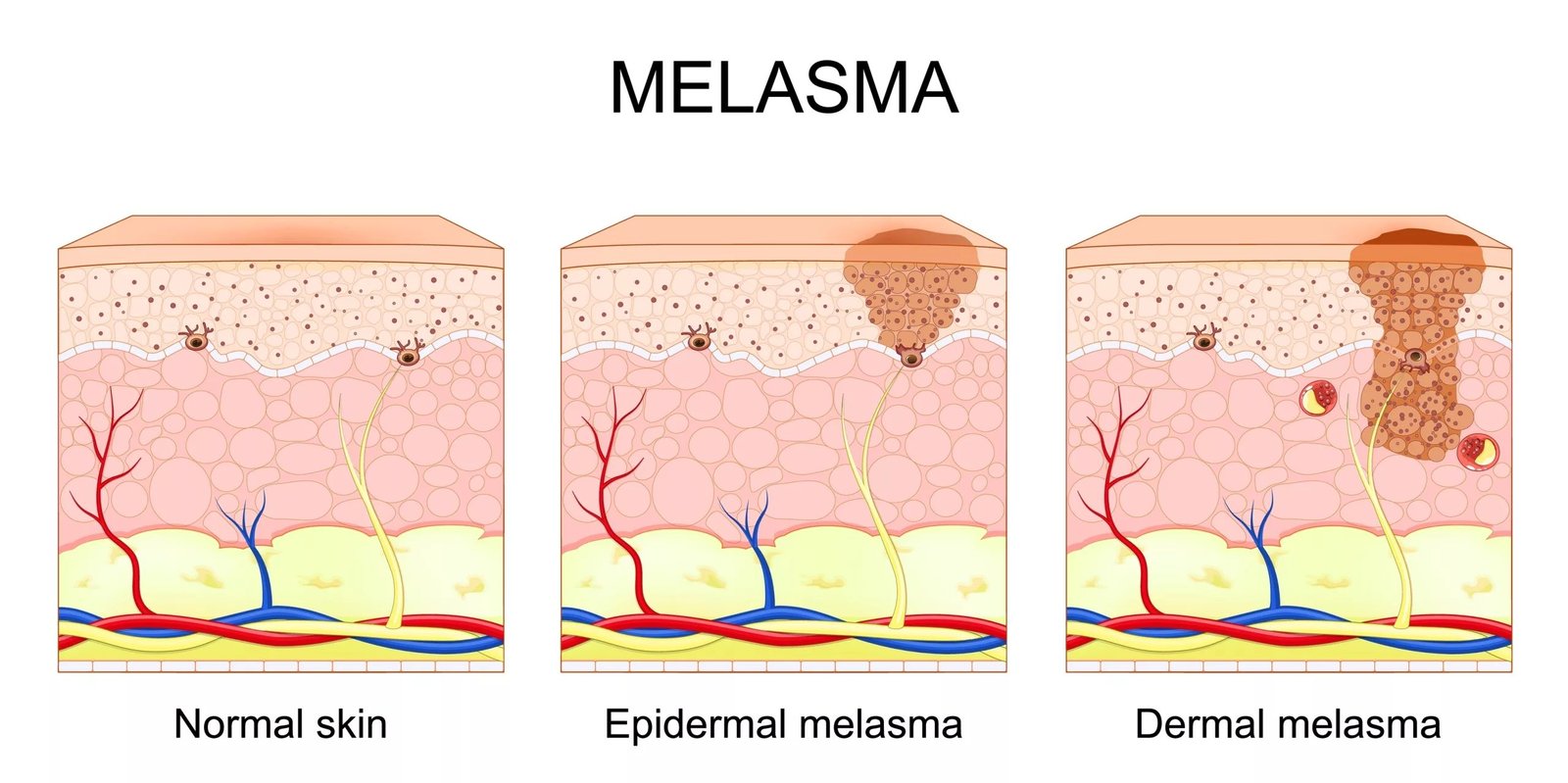
Vector Illustration showing Cross-section of human skin with Hyperpigmentation (Melasma)
Mixed-type Melasma
It presents clinically as dark brown patches. Wood’s lamp examination reveals variable enhancement, with some areas showing epidermal involvement while others demonstrate dermal pigmentation. Histologically, this subtype exhibits combined features of both epidermal and dermal melasma.
Indeterminate (Inapparent) Melasma
It is generally dark brown and may be difficult to detect clinically, particularly in individuals with skin types V–VI (dark brown or black skin). Wood’s lamp examination is typically non-contributory due to insufficient contrast. Histopathological analysis often reveals features consistent with either mixed or dermal melasma.
Clinical Features of Melasma
Melasma mostly develops in sun-exposed areas with symmetrical light or dark brownish confluent macules and patches. These are mostly on the cheeks, forehead, chin, and upper lip. Melasma lesions can be classified into three types based on their location:
- Symmetrical malar type (localized to nose and cheeks)
- Mandibular type (appears on the jawline)
- Centrofacial type (implicates cheeks, forehead, nose, chin, and upper lip)
The Centrofacial type is the most common among females, whereas the Malar type is the most frequent in males. Extra facial melasma includes symmetrical, irregular, and hyperchromic discolorations on the arms, forearms, neck, cervical, sternal, and eventually the back. It primarily affects the upper limbs in menopausal women, elderly people, and anyone receiving hormone replacement therapy. .
What Causes Melasma?
The exact cause of the disease is unknown. However, many factors can be suspected, such as genetics, pregnancy, use of cosmetics, sun exposure, oral contraceptives, and thyroid disease.
Sun Exposure
Sunlight, particularly UV radiation, is the key environmental issue that drives melasma due to its ability to intensify melanogenesis and melanocyte growth. Visible and infrared radiation also have some role, and occupational heat and bright lighting may worsen the condition. Sunscreens have UV-absorbing compounds that improve the efficacy of treatments like hydroquinone. Hormonal changes or genetic predisposition are typically necessary for melasma’s development. Additionally, autoimmune disorders and systemic conditions such as Addison’s diseaseare associated with its appearance.
Genetics
Family history is one of the significant risk factors for melasma. In a worldwide survey of 324 women, 48% showed a positive family history primarily involving first-degree relatives. Interestingly, people with lighter skin tone (Fitzpatrick skin types II and III) have a lower predisposition in the family than people with darker skin (types IV- VI). Facial melasma is usually dominantly inherited, and the factors of exposure are added to the progression of the disease in genetically susceptible people.
Hormonal factors
The hormonal factors contribute significantly to the development of melasma. It is also referred to as the mask of pregnancy because it mostly occurs in pregnant women due to hormonal changes. The hormone replacement therapy, contraceptive medications (birth control, oral contraceptive pills containing estrogen and progesterone), and hormonal imbalance can also develop hyperpigmentation.
Additionally, melasma also develops in certain hormonal conditions like thyroid disorders (especially hypothyroidism) and hormonal fluctuations related to menopause. Sometimes progesterone is prescribed to postmenopausal women, and it has been found to cause melasma. This discoloration normally fades in a few months after childbirth, after not taking oral contraceptives, managing hormonal imbalance, and minimizing exposure to sunlight. However, in many cases it persists or recurs.
Makeup (cosmetics)
Some cosmetics cause a phototoxic reaction. Perfumes, soaps, creams, powders, and shampoos containing psoralen, tar derivatives, or hexachlorophene can trigger pigmented contact dermatitis, which may mimic or worsen melasma.
Phototoxic drugs
Some phototoxic medicines (drugs that are sensitive to sunlight) also cause or worsen the melasma because it increases the sensitivity of the skin to sunlight. These include some hypoglycaemics, antibiotics, diuretics, retinoids, nonsteroidal anti-inflammatory drugs (NSAIDs), antipsychotics, targeted therapies, and some other drugs (Antiseizure drugs). Skin care products and scented soaps also worsen pigmentation..
Diagnosis of Melasma
Melasma is primarily a clinical diagnosis based on history and characteristic skin findings. Patients typically present with symmetrical, light- to dark-brown macules and patches on sun-exposed areas, particularly the face. A detailed history should assess potential triggers such as sun exposure, hormonal factors (e.g., pregnancy or oral contraceptive use), medications, and cosmetic products.
Adjunctive tools may be used to support the diagnosis and assess the depth of pigmentation. A Wood’s lamp examination can help differentiate epidermal from dermal pigmentation, although its reliability is limited, especially in individuals with darker skin types. Dermoscopy is increasingly used in clinical practice, as it provides better visualization of pigment patterns and vascular changes. In selected cases, reflectance confocal microscopy or histopathological examination may be considered, particularly when the diagnosis is uncertain.
Severity assessment tools such as the Melasma Area and Severity Index (MASI) are commonly used in research settings and can help monitor treatment response over time.
Differential Diagnosis of Melasma
Melasma should be differentiated from other causes of facial hyperpigmentation, particularly those presenting with symmetrical or photo-distributed pigmentation.
| Condition | How it differs from melasma |
|---|---|
| Post-inflammatory hyperpigmentation | Follows acne or skin injury; irregular, non-symmetrical pigmentation |
| Pigmented contact dermatitis | Associated with cosmetics or fragrances; diffuse gray-brown pigmentation, sometimes itchy |
| Exogenous ochronosis | Linked to long-term hydroquinone use; blue-black, mottled pigmentation |
| Lichen planus pigmentosus | Diffuse slate-gray pigmentation with poorly defined borders |
| Discoid lupus erythematosus | Redness, scaling, scarring, and photosensitivity |
| Acanthosis nigricans | Velvety thickened skin, mainly on neck and flexures |
| Nevus of Ota / Ito | Bluish-gray pigmentation, usually unilateral and present from early life |
| Drug-induced pigmentation | History of medication use; variable pattern and distribution |
| Poikiloderma of Civatte | Neck involvement with redness, atrophy, and visible blood vessels |
Management and Treatment of Melasma
Melasma is a chronic and relapsing disorder, and management focuses on controlling pigmentation, preventing progression, and minimizing recurrence. There is no specific medication to treat melasma yet. However, several medicines and surgeries can be used to treat this disorder. To determine a treatment plan, your doctor first figures out what’s causing the melasma. Genetics? Your birth control? Is it sunlight? Your soap? More screen time?
It may be permanent, may respond to treatment within a few months, or it may go away on its own, depending on the person. The majority of the cases will disappear over time, particularly with proper protection against sunlight and other light sources.
General Measures and Photoprotection
The first step in treating your uneven skin toneis to ensure that it does not get any worse. This can be done by avoiding the sun, irritating soaps, LED screens, and birth control, which has hormones. Broad-spectrum sunscreen (SPF ≥30) should be used daily and reapplied regularly, especially during outdoor exposure.
Protective measures such as wide-brimmed hats and avoiding peak sunlight hours are also recommended.
Patients should also avoid known aggravating factors such as tanning beds, unnecessary heat exposure, and irritating cosmetic products.
Topical Therapy
Topical agents are the mainstay of treatment. The most effective regimen is triple combination therapy, which includes hydroquinone, tretinoin, and a mild to moderate topical corticosteroid
Other commonly used topical agents include azelaic acid, kojic acid, cysteamine, and vitamin C. These agents act through tyrosinase inhibition and antioxidant effects and can be used alone or as adjuncts.
Oral Therapy
Sometimes, when melasma is associated with a hormonal deficit, a dermatologist may prescribe oral drugs that will balance hormone levels and reduce melasma symptoms. However, care must be taken because there are side effects to these drugs, and they should be used only in case the doctor believes it is necessary.
In some situations, it can be recommended to stop taking some medications or hormonal contraceptives in case they cause the development of melasma.
Tranexamic acid has emerged as an effective adjunct therapy. It inhibits the conversion of plasminogen to plasmin and downstream signaling prevents the synthesis of prostaglandin and other elements in melasma. However, it is used off-label and should only be prescribed after careful patient evaluation due to the potential risk of thromboembolic complications. More new oral treatments are under trial.
Procedural Treatments
Procedural options may be considered in patients who do not respond adequately to topical therapy. These include chemical peels, laser therapy, and intense pulsed light (IPL).
Superficial chemical peels using glycolic acid or salicylic acid help in epidermal exfoliation and pigment reduction. Laser and light-based therapies can be effective in selected cases but must be used cautiously, particularly in darker skin types, due to the risk of post-inflammatory hyperpigmentation and recurrence.
Pretreatment with topical depigmenting agents is often recommended to improve outcomes and reduce complications.
Long-term Management
Melasma is a chronic condition with a high tendency for recurrence. Therefore, long-term maintenance therapy and strict photoprotection are essential even after clinical improvement. Patient counseling is important to set realistic expectations regarding treatment duration and outcomes.
Is it possible to avoid melasma?
However, it is not possible to completely prevent melasma, especially in genetically predisposed individuals or during pregnancy. Nevertheless, you can avoid factors that exacerbate melasma. Strict photoprotection remains the most effective preventive measure.
Bottom line
Melasma is a common, harmless, and chronic skin disorder that can significantly affect quality of life. It may impact social confidence and emotional well-being. However, effective management strategies are available. Always follow your healthcare provider’s advice and adhere to long-term treatment and photoprotection plans.
References
[1] R, D. K., Sood, R., & Tiwari, P. (2025). Melasma management: Unveiling recent breakthroughs through literature analysis.Health Sciences Review,14, 100213. https://doi.org/10.1016/j.hsr.2025.100213
[2] Kauh, Y. C., & Zachian, T. F. (1999). Melasma.Rheumaderm, 491–499. https://doi.org/10.1007/978-1-4615-4857-7_72
[3] Kauh, Y. C., & Zachian, T. F. (1999). Melasma.Rheumaderm, 491–499. https://doi.org/10.1007/978-1-4615-4857-7_72
[4] Sarkar, R., Ghunawat, S., Narang, I., Verma, S., Garg, V. K., & Dua, R. (2019). Role of broad‐spectrum sunscreen alone in the improvement of melasma area severity index (MASI) and Melasma Quality of Life Index in melasma.Journal of Cosmetic Dermatology,18(4). https://doi.org/10.1111/jocd.12911
[5] View of Melasma Clinical Features, Diagnosis, Epidemiology and Etiology: An Update Review. (2024). Tci-Thaijo.org. https://he02.tci-thaijo.org/index.php/sirirajmedj/article/view/255148/173335
[6] Tamega, A. de.A., Miot, L. D. B., Bonfietti, C., Gige, T. C., Marques, M. E. A., & Miot, H. A. (2012). Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women.Journal of the European Academy of Dermatology and Venereology,27(2), 151–156. https://doi.org/10.1111/j.1468-3083.2011.04430.x
[7] D’Elia, M. P. B., Brandão, M. C., de Andrade Ramos, B. R., da Silva, M. G., Miot, L. D. B., dos Santos, S. E. B., & Miot, H. A. (2017). African ancestry is associated with facial melasma in women: a cross-sectional study.BMC Medical Genetics,18(1). https://doi.org/10.1186/s12881-017-0378-7
[8] Neel Prabha, Mahajan, V. K., Mehta, K. S., Chauhan, P. S., & Gupta, M. (2014).Cosmetic Contact Sensitivity in Patients with Melasma: Results of a Pilot Study.2014, 1–9. https://doi.org/10.1155/2014/316219
[9] View of Melasma Clinical Features, Diagnosis, Epidemiology and Etiology: An Update Review. (2024). Tci-Thaijo.org. https://he02.tci-thaijo.org/index.php/sirirajmedj/article/view/255148/173335
[10] McKesey, J., Tovar-Garza, A., & Pandya, A. G. (2019). Melasma Treatment: An Evidence-Based Review.American Journal of Clinical Dermatology,21(2). https://doi.org/10.1007/s40257-019-00488-w
[11] Jiryis, B., Toledano, O., Avitan-Hersh, E., & Khamaysi, Z. (2024). Management of Melasma: Laser and Other Therapies—Review Study.Journal of clinical medicine,13(5), 1468.