
{kind=link}

Behcet’s disease (BD), also known as Silk Road disease, is a rare disorder characterized by chronic inflammation of the blood vessels, i.e., vasculitis. It causes recurrent ulcers (sores) in the oral and genital regions, with body aches and eye issues. The disorder affects both arteries and veins of all sizes, thereby making it a disease with high morbidity and potentially serious complications in severe cases. Experts believe that the disease arises due to an autoimmune-mediated attack on the vascular tissues.
According to a study, the prevalence of Behcet’s disease in the US was found to be 0.33 to 5.2/100,000 people, while a higher prevalence is seen in countries like Turkey, Iran, China, etc. The disease shows geographic variation in sex distribution. In Middle Eastern and Mediterranean countries, it is more common in males, whereas in Western countries, females may be slightly more affected. It can affect people of all ages, but symptoms typically begin to appear between the ages of 20 and 30.
Genetic and environmental factors are believed to play a role in the pathogenesis of the vascular disorder. There is no known cure for the disease. However, doctors manage the disease with corticosteroids and immunosuppressant drugs.
Symptoms Of Behcet’s Disease
As the disease can affect arteries and veins all over your body, a wide array of symptoms is seen. Therefore, most patients have to consult different specialists with the multitude of problems.
The most common symptoms of Behcet’s disease include:
Mouth Ulcers
According to clinicians, the most frequent symptom of the vascular disease is mouth ulcers or sores. Many patients experience non-specific oral presentations associated with the disease. It has been reported in 80-95% of cases. A 2023 study concluded oral manifestations to be the primary symptoms of BD. Many times, oral ulcers develop long before any other symptoms of the disease appear.
Orogenital ulcers develop when the disease affects the vessels of the mucous membranes of the body. The Behcet’s oral sores are similar to common canker sores. However, you will find them in greater numbers spread to different oral regions. According to the majority of patients, these sores/ulcers cause pain and discomfort when talking, eating, and brushing. This leads to a reduction in oral health-related quality of life. The most common sites of ulcers/sores are:
- Lips
- Tongue
- Inside the cheek

Close-up of a recurrent oral ulcer on the lip of a patient.
A salient feature of the disease is that these ulcers recur. As per clinical studies, painful recurrent mouth ulcers are present in all patients. The sores begin as raised (round) lesions that quickly become painful. Recurrent apthous ulcers are seen on the tongue and inner cheeks.
Genital Ulcers
Ulcerations are not limited to the oral region. Several patients suffer from genital ulcers. These lesions are similar to mouth ulcers, are recurrent, and can be painful. However, they are not as common as their oral counterparts. Many healthcare providers suspect the Silk Road disease if a patient presents with recurrent orogenital ulcers.
The majority of genital ulcers heal by scarring. In women, sores appear on external genital organs like the vulva, vagina, and cervix, while in men, most ulcers (around 90%) are present on the scrotum (sack covering the testicles). Vulva ulcers can lead to tissue loss. Therefore, these ulcers can negatively impact intimate relationships.
Eye Issues
This systemic vascular disease can also affect the fine blood vessels of your eyes. Many individuals suffer from eye pain and blurry vision. Inflammation of the middle layer of the eye, uveitis, is the most prevalent ocular (eye) manifestation of the disease. Uveitis can develop on the front of the eye (anterior uveitis) or on the back side (posterior uveitis). According to a 2021 study, uveitis can be an initial symptom in about 10-20% cases. It can lead to blindness in 16-25% of patients.
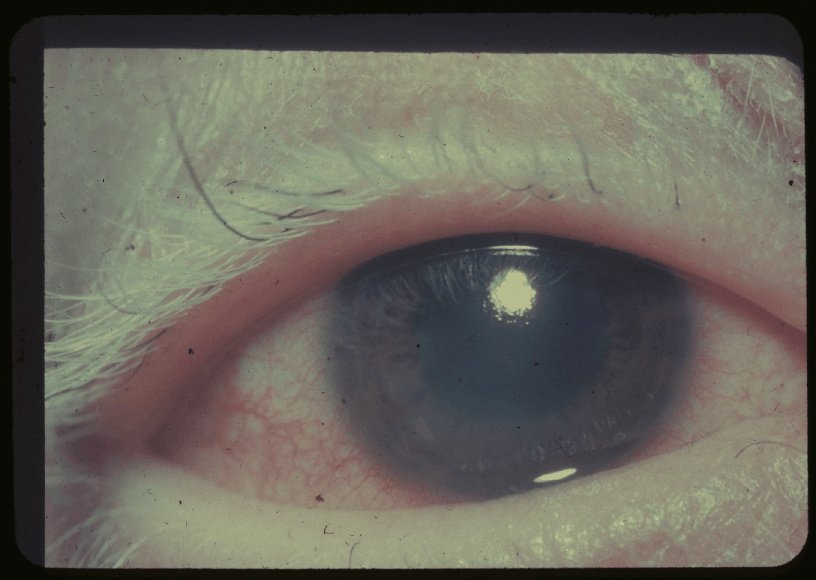
Close-up of the eye of a Behcet’s disease patient showing redness due to uveitis.
Patients also report having light sensitivity with eye redness and increased production of tears. Behcet’s-induced uveitis can cause symptoms like periocular pain, eye redness, and photophobia (fear of lights).
Bechet’s disease may even lead to vision loss and blindness. Research shows that recurrent inflammation of the vessels in the retina (light-sensitive, innermost layer), i.e., retinal vasculitis, potentially causes severe ocular damage, which can lead to blindness.
Body Aches
Another issue arising from Behcet’s disease is chronic body aches, which are attributed to joint inflammation. Approximately 30-60% of patients exhibit joint symptoms. Studies show that the disease predominantly causes joint pain (arthralgia) in the peripheral joints (hips, knees, ankles, etc.).
According to a study conducted in Japan, noticeable swelling and pain were present in the knee, ankle, and finger joints. In most cases, episodes of pain/swelling last for 1 to 3 weeks. However, like the orogenital ulcers, the symptoms come and go. It may affect one or more joints at the same time, i.e., polyarthralgia.
Skin Problems
In addition to the mucosal sores, dermatological consequences of the systemic disorder are also noticeable. In the majority of cases with skin involvement, Behcet’s causes the development of red nodules on the skin (in 15-78% of cases). These coin-shaped nodules resemble a skin disorder, erythema nodosum. The erythema nodosum-like (EN-like) lesions are painful, tender, and seen on the upper/lower extremities (limbs) and face/neck region.

Erythematous (red) papules on the patient’s legs caused by underlying vasculitis.
Pseudofolliculitis is another major cutaneous sign of the syndrome. It is characterized by the formation of a red papule (raised, solid skin lesion) that resembles acne. The papule gradually changes into a clear pustule (small, pus-filled blister). This is also painful, tender, and can be itchy at times.
Vasculitis
Vein inflammation (vasculitis) can have a variety of negative effects on the entire body. A unique feature of this syndrome is that it affects vessels of all sizes (from small to medium to large). The impact on pulmonary (lung) veins contributes to disease mortality.
Involvement of the deeper, large vessels, like the vena cavae (veins that return blood to the heart), can potentially lead to serious health problems. The disease is known to cause blockage (by forming blood clots) of major arteries and veins, as well as narrowing and bulging in the artery walls.
Neuro-Behcet’s Disease
Healthcare givers call the combination of neurologic symptoms Neuro-Behcet’s disease (NBD). Researchers have noted frequent involvement of the brain parenchyma (brain tissue itself), which can lead to life-threatening inflammation. Neuro-Behcet’s can be classified into parenchymal and non-parenchymal forms, the latter often involving cerebral venous sinus thrombosis. Meningitis and encephalitis may occur in some patients.
Common symptoms of brain involvement include fever, headache, and neck stiffness. Due to the brain tissue inflammation, a lot of patients lose control over their bodies and have difficulty coordinating movement. Hemorrhages can also be seen in such cases. The vast majority of patients report having fatigue, which usually does not respond to conventional treatment.
Gastrointestinal Disturbance
You can feel symptoms of the disease in your GI tract. There have been reports of abdominal pain and blood in the stool. These symptoms are attributed to the development of mucosal ulcers in the tract. However, GI lesions pose greater problems than the orogenital disease as they can lead to rupture and bleeding of the intestine.
Involvement of the vessels of crucial organs like the kidneys can have grave consequences. Pulmonary vessels and large vessels like the aorta can occasionally be affected, which can contribute to serious adverse effects.
Behcet’s Disease Causes
No one knows the exact cause of this syndromic vascular disorder. However, most scientists believe it is an autoimmune disorder in which the body’s defense system (immune system) mistakenly attacks healthy vessels, leading to inflammation. Researchers have recognized genetic and non-genetic factors at play.
Genetics
Researchers have identified certain gene/genetic markers linked to Behcet’s disease. Genetic markers are specific sequences of DNA on your chromosomes that are linked to inherited diseases. HLA-B5 and HLA-B51 are gene markers that are sometimes present in Behcet’s patients. Studies show that carriers of the HLA-B51 allele have a 6-10 fold higher risk of developing Behcet’s. 50-80% of patients belonging to the Silk Road nations showed positive gene markers, while only a small percentage (about 15%) of patients in the US/Europe carried the allele. This means only a small percentage of US patients have the gene markers for Behcet’s disease.
There are non-HLA genes (ERAP1, IL-10, and IL23R/IL-12RB2) that are linked to the disorder. Moreover, genes that control innate immunity (FUT2, MICA, TLRs) also contribute to the disease.
Environmental Factors
Clinicians don’t fully understand how environmental factors contribute to the disease. But it has been observed that the disease develops in response to the co-occurrence of genetic and environmental factors. Some researchers think that infection (bacterial or viral) can act as a trigger for the disease (in patients having a genetic predisposition). Certain infections are known to trigger the disease or exacerbate symptoms. Pathogens frequently associated with the syndrome include Streptococcus spp, herpes simplex virus, parvovirus, etc.
Risk Factors
The following groups are at a higher risk of developing the disease:
- Middle-aged men (20 to 40 year olds)
- Residents of the Silk Road Nations (China, Turkey, Pakistan, Kazakhstan, etc.)
- Individuals carrying HLA-B5 and HLA-B51 genes
Behcet’s Disease Diagnosis
Due to the widespread symptoms and presentations, doctors use different tests to reach a diagnosis. Your healthcare provider will begin by physically examining the orogenital ulcers and taking a history of the onset of symptoms. He may also ask you about the family history of the syndrome.
ISG Diagnostic Criteria
Most doctors use the International Study Group (ISG) criteria to diagnose Behcet’s disease. The main diagnostic feature according to this criterion is the presence of recurrent oral ulcers that occur at least 3 times in a year. A person is considered to be suffering from the vascular disease if they have any 2 or more of the following symptoms:
- Recurrent genital sores/ulcers
- Eye lesions (anterior or posterior uveitis)
- Skin lesions (erythema-nodosum-like lesions or pseudofolliculitis)
- A positive pathergy test
ICBD Criteria
A more accurate criterion is the International Criteria for Behcet’s disease (ICBD). This criterion allocates points to the various symptoms that help determine the severity of the disorder. The scoring criteria are as follows:
- Oral ulcers: 2 points
- Genital sores/ulcers: 2 points
- Eye lesions: 2 points
- Skin lesions: 1 point
- Neurological symptoms: 1 point
- Vascular manifestations: 1 point
- Positive pathergy test: 1 point
A score of ≥4 is diagnosed as Behcet’s disease. ICBD is more accurate and sensitive than ISG.
Pathergy Test
A pathergy test is done to check a person’s immune system’s functionality. In this diagnostic procedure, the doctor pricks the patient’s forearm with a fine, sterile needle. The test is positive if a red bump, pustule, or ulcer develops on the needle prick site after a few days (24-48 hours later), indicating a hypersensitive immune response. A positive pathergy test supports the diagnosis but does not independently confirm it, as the diagnosis remains clinical.
Your doctor may also order blood tests and imaging studies (CT, MRI scans) to rule out similar pathologies like Crohn’s disease and systemic lupus erythematosus.
Differential Diagnosis
Different diseases fall under the DD of Behcet disease. The Silk Road disease has presentations similar to lupus.
Behcet’s Disease Vs Systemic Lupus Erythematosus
Both diseases present with skin lesions and body aches. However, we see recurrent orogenital ulcers with uveitis in BD, while a typical malar rash and positive autoimmune serologies are seen in SLE. A pathergy test is typically negative in SLE.
Behcet’s Disease Treatment
There is no definitive treatment or cure for Behcet’s disease. However, a combination of different medicinal drugs has shown promise in halting the disease progression and improving symptoms.
Medicines
A variety of drugs are advised for patients displaying different symptoms of the disease. Most commonly prescribed drugs include:
Corticosteroids:
Steroid medicines like prednisolone are frequently advised to autoimmune patients. These drugs reduce inflammation and suppress the overactive immune system. According to a study, corticosteroids and immunosuppressant drugs improve BD-induced conditions, including vasculitis, GI symptoms, neurologic symptoms, and eye symptoms, etc.
Colchicine:
It is primarily used to alleviate or prevent flare-ups of gouty arthritis. It has a notable anti-inflammatory profile. Therefore, it is used in BD. It was concluded in a 2023 study that colchicine reduces the severity of symptoms and improves the overall disease activity index.
Immunosuppressants:
A wide variety of immunosuppressant drugs are available nowadays. Among the different classes, Disease Modifying Anti-Rheumatic Drugs (DMARDs) are most commonly prescribed. DMARDs work by inhibiting specific components of the immune system.
Azathioprine is the first-line immunosuppressant drug that improves uveitis symptoms. Cyclosporine A can be used in combination with a biologic drug to manage refractory eye problems. Methotrexate is useful, but is contraindicated in pregnant women.
Biologics
Biologics are a new class of drugs that are pretty effective in a wide array of autoimmune disorders. Infliximab and Tocilizumab are reserved for more severe cases. These drugs provide relief by blocking the inflammatory pathways. Tumor necrosis factor is a pro-inflammatory chemical that promotes inflammation in autoimmune disorders. Anti-TNF drugs like infliximab and adalimumab are efficient in treating Behcet’s patients (especially intestinal symptoms and uveitis).
Modern studies advocate the use of tocilizumab as it effectively improves ocular, vascular, and neurological symptoms of the disease.
Symptomatic Management
For symptomatic management, your doctor may advise eye drops for uveitis, mouthwashes for oral ulcers, and ointments for skin lesions, etc.
Final Word
Behcet’s disease is a syndrome characterized by a wide array of symptoms that are attributed to chronic inflammation of blood vessels (arteries, veins, etc) of all sizes. Patients commonly report recurrent orogenital ulcers/sores, uveitis (eye layer inflammation), and subsequent vision loss, polyarthralgia (multiple joint aches), erythematous (red) and painful skin lesions, and neurological complications like meningoencephalitis (swelling of brain tissue and layers). Some patients also experience gastrointestinal disturbances, cardiovascular issues, and kidney problems. The disease is common in Silk Road nations, including China, Turkey, Pakistan, etc.
The exact cause is unknown, but it is believed that the disease is an autoimmune disorder (in which the body’s defense system mistakenly destroys its own cells). Numerous studies have identified specific gene markers in the DNA, i.e., HLA-B5 and HLA-B51, associated with the disease. These genetic factors are triggered by environmental factors like infection.
Doctors use the ICBD criteria to diagnose the condition. A positive pathergy test confirms the diagnosis of Behcet’s disease. Healthcare professionals manage the symptoms with corticosteroids and colchicine. Immunosuppressants like azathioprine calm down the overactive immune system and halt disease progression. Other similar drugs include cyclosporine A and methotrexate. For severe, refractory cases, dermatologists/rheumatologists advise biologics like infliximab and adalimumab. Drugs like tocilizumab and infliximab have shown excellent results in alleviating symptoms.
References
[1] Hammam, N., Li, J., Evans, M., Kay, J. L., Izadi, Z., Anastasiou, C., … & Schmajuk, G. (2021). Epidemiology and treatment of Behçet’s disease in the USA: insights from the Rheumatology Informatics System for Effectiveness (RISE) Registry with a comparison with other published cohorts from endemic regions.Arthritis research & therapy,23(1), 224.
[2] Sakane T, Takeno M, Suzuki N, Inaba G. Behçet’s disease.N Engl J Med.1999;341(17):1284–1291.
[3] Soares, A. C., Pires, F. R., de Oliveira Quintanilha, N. R., Santos, L. R., Amin Dick, T. N., Dziedzic, A., & Picciani, B. L. S. (2023). Oral lesions as the primary manifestations of Behçet’s disease: the importance of interdisciplinary diagnostics—a case report.Biomedicines,11(7), 1882.
[4] Ali, S., Nagieb, C. S., & Fayed, H. L. (2023). Effect of Behcet’s disease‐associated oral ulcers on oral health related quality of life.Special Care in Dentistry,43(4), 435-442.
[5] Kudsi, M., Khalayli, N., & Allahham, A. (2022). Behcet’s disease: Diagnosed as isolated recurrent oral aphthae; a case report.Annals of Medicine and Surgery,81, 104327.
[6] Narang, S. K., & Shah, H. A. (2024). Behcet syndrome: A rare cause of recurrent genital ulceration.Indian Journal of Sexually Transmitted Diseases and AIDS,45(2), 156-159.
[7] Nakamura, K., Tsunemi, Y., Kaneko, F., & Alpsoy, E. (2021). Mucocutaneous manifestations of Behçet’s disease.Frontiers in medicine,7, 613432.
[8] Sweeting, F., & Arden-Close, E. (2022). The impact of Behcet’s disease on intimate relationships in women: a qualitative study.Chronic illness,18(2), 255-267.
[9] Zając, H., & Turno-Kręcicka, A. (2021). Ocular manifestations of Behçet’s disease: an update on diagnostic challenges and disease management.Journal of clinical medicine,10(21), 5174.
[10] Marieta, D., & Rodica, L. (2022). Eye Manifestations in Behcet’s Syndrome.Journal of Clinical Medicine & Surgery,1(1), 5.
[11] Ksiaa, I., Abroug, N., Kechida, M., Zina, S., Jelliti, B., Khochtali, S., … & Khairallah, M. (2019). Eye and Behçet’s disease.Journal francais d’ophtalmologie,42(4), e133-e146.
[12] Mohamadi, A., Karimi, E., Nayebirad, S., Yousefi-Koma, H., Karimi, Z., Tamartash, Z., … & Kavosi, H. (2025). The trends in the prevalence of arthritis and arthralgia and their associations with extra-articular manifestations in patients with Behcet’s disease: A systematic review and meta-analysis.Modern Rheumatology,35(6), 1015-1029.
[13] Tono, T., Kikuchi, H., Sawada, T., Takeno, M., Nagafuchi, H., Kirino, Y., … & Hirohata, S. (2022). Clinical features of Behçet’s disease patients with joint symptoms in Japan: A national multicenter study.Modern Rheumatology,32(6), 1146-1152.
[14] Scherrer, M. A. R., Rocha, V. B., & Garcia, L. C. (2017). Behcet’s disease: review with emphasis on dermatological aspects.Anais brasileiros de dermatologia,92(4), 452-464.
[15] Pak, D., & Park, H. J. (2023). Behcet disease: an undifferentiating and complex vasculitis.Postgraduate Medicine,135(sup1), 33-43.
[16] Alpagut, U., Ugurlucan, M., & Dayıoglu, E. (2007). Major arterial involvement and review of Behcet’s disease.Annals of vascular surgery,21(2), 232-239.
[17] Belfeki, N., Ghriss, N., Fourati, M., Leclercq, D., & Saadoun, D. (2024). Neuro-Behçet’s disease: A review.La Revue de Médecine Interne,45(10), 624-633.
[18] Nguyen, A., Upadhyay, S., Javaid, M. A., Qureshi, A. M., Haseeb, S., Javed, N., … & Sheikh, A. B. (2021). Behcet’s disease: an in-depth review about pathogenesis, gastrointestinal manifestations, and management.Inflammatory Intestinal Diseases,6(4), 175-185.
[19] Khoshbakht, S., Başkurt, D., Vural, A., & Vural, S. (2023). Behçet’s disease: a comprehensive review on the role of HLA-B* 51, antigen presentation, and inflammatory cascade.International Journal of Molecular Sciences,24(22), 16382.
[20] Moghoofei, M., Pajavand, H., Shahbazi, R., Rezaei, M., & Taki, E. (2026). The Role of Viral and Bacterial Infections in the Etiology of Behçet’s Disease.Journal of Clinical Laboratory Analysis,40(1), e70133.
[21] Davatchi, F. (2012). Diagnosis/Classification Criteria for Behcet′ s Disease.Pathology research international,2012(1), 607921.
[22] Alpsoy, E., Leccese, P., Emmi, G., & Ohno, S. (2021). Treatment of Behçet’s disease: an algorithmic multidisciplinary approach.Frontiers in medicine,8, 624795.
[23] Wang, Z., Zu, X., Xiong, S., Mao, R., Qiu, Y., Chen, B., … & He, Y. (2023). The role of colchicine in different clinical phenotypes of Behcet disease.Clinical therapeutics,45(2), 162-176.
[24] Alibaz-Oner, F., & Direskeneli, H. (2021). Advances in the treatment of Behcet’s disease.Current rheumatology reports,23(6), 47.
[25] Katsuyama, A., Kusuhara, S., Nishisho, R., Matsumiya, W., Azumi, A., & Nakamura, M. (2019). Long-term efficacy and safety of infliximab and cyclosporine combination therapy for refractory uveoretinitis in Behçet’s disease.Clinical Ophthalmology (Auckland, NZ),13, 521.
[26] Zhang, M., Liu, J., Liu, T., Han, W., Bai, X., Ruan, G., … & Qian, J. (2022). The efficacy and safety of anti‐tumor necrosis factor agents in the treatment of intestinal Behcet’s disease, a systematic review and meta‐analysis.Journal of Gastroenterology and Hepatology,37(4), 608-619.
[27] Takeuchi, M., Usui, Y., Namba, K., Keino, H., Takeuchi, M., Takase, H., … & Goto, H. (2023). Ten-year follow-up of infliximab treatment for uveitis in Behçet disease patients: A multicenter retrospective study.Frontiers in Medicine,10, 1095423.
[28] Akiyama, M., Kaneko, Y., & Takeuchi, T. (2020, August). Effectiveness of tocilizumab in Behcet’s disease: a systematic literature review. InSeminars in Arthritis and Rheumatism(Vol. 50, No. 4, pp. 797-804). WB Saunders.