
{kind=link}

Budd Chiari Syndrome Budd-Chiari syndrome is a rare condition defined as hepatic venous outflow obstruction that is not caused by cardiac or pericardial disease. It is classified into primary and secondary Budd-Chiari syndrome. The overall incidence is estimated at approximately 0.5–1 case per million people per year, with regional variations. Primary Budd-Chiari syndrome is a rare condition. In primary Budd-Chiari syndrome, obstruction is usually due to thrombosis or phlebitis originating within the hepatic veins themselves. Secondary Budd-Chiari syndrome is a compression or invasion of the hepatic veins of the inferior vena cava by a lesion that originates outside the vein. The disorder presents in acute, subacute, and chronic forms. Symptoms include abdominal pain, ascites, and hepatomegaly.
Causes of Budd-Chiari Syndrome: Budd Chiari Syndrome
In up to 80% of cases, some underlying prothrombotic causes lead to the development of Budd-Chiari syndrome.
Myeloproliferative Disorders
About half of the cases of this condition occur in patients with myeloproliferative disorders (essential thrombocythemia and polycythemia vera). The presence of the JAK2 V617F mutation is frequently identified and should be actively investigated, even in patients previously labeled as idiopathic. This is because some hypercoagulability almost always accompanies these myeloproliferative disorders.
Malignancy
Around 10% of cases are due to malignancy, which can cause either direct vessel invasion or compression.Malignancy, along with hypercoagulability, leads to obstruction and venous thrombosis. The common cancers related to Budd-Chiari syndrome are hepatocellular carcinoma. Other malignancies, such as renal cell carcinoma, adrenal tumors, leiomyosarcoma, and rarely right atrial myxoma or Wilms tumor, have also been reported.
Pregnancy and Oral Contraceptives
Pregnancy and oral contraceptives are responsible for about 20% of the cases of Budd-Chiari syndrome, as they lead to a hypercoagulable state.
Benign Lesions of the Liver
A space-occupying liver lesion or infection may compress the vasculature, leading to this disorder. Hepatic cysts, invasive aspergillosis, cystadenomas, and aortic lesions can also lead to Budd-Chiari syndrome.
Idiopathic
An estimated 20% of the Budd-Chiari syndrome cases are idiopathic. However, many of these patients are later found to have occult thrombophilic disorders, including myeloproliferative disease or inherited coagulation abnormalities.
Additional Causes
Some other hypercoagulable states responsible for this condition are:
- Protein C deficiency
- Antithrombin deficiency
- Paroxysmal nocturnal hemoglobinuria
- Antiphospholipid antibody syndrome
- Factor V Leiden mutation, causing resistance to activated protein C
Pathophysiology of Budd-Chiari Syndrome
Occlusion of a single hepatic vein remains silent, but when two hepatic veins are occluded, venous congestion stretches the liver capsule, causing severe abdominal pain. The sinusoids begin to dilate, and interstitial fluid infiltration leads to hepatic congestion. When lymphatic drainage is overwhelmed, fluid leaks through the liver capsule into the peritoneal cavity, producing ascites. Prolonged hepatic venous obstruction results in centrilobular hypoxia, ischemic necrosis, and progressivefibrosis. All these activities eventually result in portal hypertension and ascites.
In chronic disease, some parts of the liver adapt better than others. The caudate lobe often enlarges because it continues to drain blood more effectively, even when other veins are blocked. Acute blockage can cause sudden and severe liver failure, while long-standing disease usually progresses more slowly, with an enlarged liver and fluid buildup but relatively preserved liver function.
Clinical Presentation and Symptoms of Budd-Chiari Syndrome
Most of the patients present with the classic triad of hepatomegaly, ascites, and abdominal pain. Based on clinical presentation and condition severity, Budd-Chiari syndrome is classified into three types.
Acute Budd-Chiari Syndrome
The clinical manifestations develop rapidly over a few weeks, with hepatic necrosis and intractable ascites. In this type, fulminant liver failure can occur. It is characterized by acute liver injury along with elevated transaminases, prolonged prothrombin time, jaundice, and hepatic encephalopathy.
Chronic Budd-Chiari Syndrome
Patients present with complications of portal hypertension and cirrhosis, including venous collaterals, splenomegaly, and progressive liver dysfunction.
Subacute Budd-Chiari Syndrome
Subacute manifestations of this condition have an insidious onset, with patients taking up to three months to develop the symptoms of venous collaterals, leading to minimal ascites and hepatic necrosis.

Symptoms of Budd-Chiari syndrome
Diagnosis of Budd-Chiari Syndrome
Due to the non-specific nature of the findings and a wide range of clinical presentations, there is a high degree of suspicion for diagnosing the disease. No individual test establishes the diagnosis of Budd-Chiari syndrome. Diagnosis is based on the classical clinical manifestations and conditions predisposed to thrombosis.
Physical Examinations and History
Clinicians observe the following presentations on physical examination of patients with Budd-Chiari syndrome:
- Ascites
- Jaundice
- Hepatomegaly (Enlarged liver)
- Pedal edema
- Splenomegaly
- Stasis ulcerations (stasis-related skin changes)
Clinicians also suspect Budd-Chiari syndrome on observing the following things:
- Massive ascites with normal liver function
- Sudden onset of ascites and painful hepatomegaly
- Unexplained chronic liver disease
- Sinusoidal dilation in liver biopsy
Imaging Tests
Color Doppler ultrasound is the initial imaging modality, with a reported sensitivity and specificity of approximately 85–90%, depending on operator expertise. Its typical findings include:
- Ascites
- Inferior vena cava webs or stenosis
- Increased caudate lobe size
- Presence of hepatic venous thrombosis
- Presence of extrahepatic and intrahepatic collaterals
- Decreased IVC diameter
- Remarkably high velocity in areas of stenosis
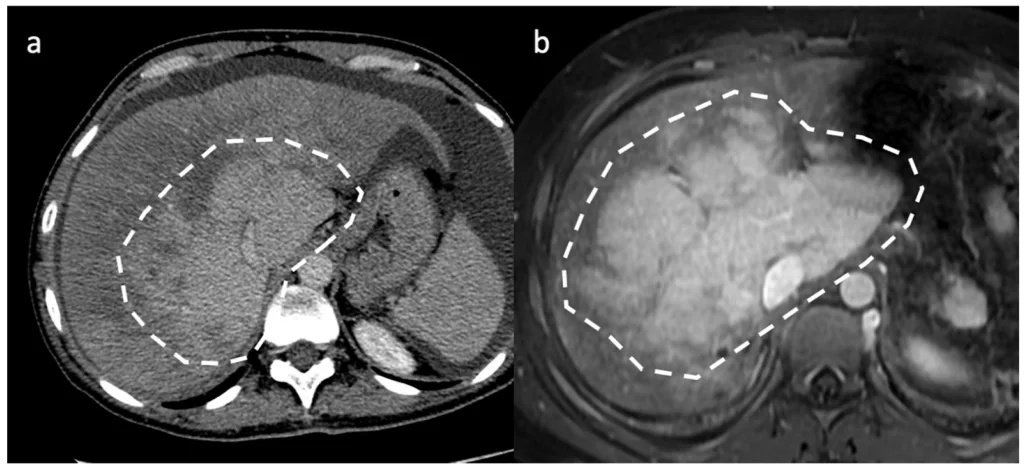
Two different cases of acute/subacute BCS. On axial portal venous phase CT (a) and MR (b) images, the liver exhibits decreased peripheral enhancement caused by portal and sinusoidal stasis, with stronger central liver enhancement, a pattern called “zonal enhancement” (white circles). Image Courtesy: Budd-Chiari Syndrome Imaging Diagnosis: State of the Art and Future Perspectives by Porrello et al, 2023,doi.org/10.3390/diagnostics13132256, available via: MDPI, CC BY 4.0.
A CT scan is helpful when mechanical obstruction is present as an underlying cause. MRI can also aid in diagnosis with a sensitivity and specificity of >90 percent.
Venography is beneficial if these tests fail to establish the diagnosis. It can accurately show the sites and severity of the obstruction. However, its invasive nature limits its use. Liver elastography may demonstrate increased liver stiffness due to congestion rather than fibrosis, which should be interpreted cautiously.
Paracentesis and Laboratory Evaluation
Paracentesis is a procedure in which a doctor inserts a needle into the abdomen to collect a sample of ascitic fluid for lab tests. Labs are typically ordered to assess liver function. Elevated protein levels >2g/dL and white blood cells <500/µL are usually present in patients with chronic disease. Mild elevations in serum aminotransferase and alkaline phosphate levels are found in almost half of the patients with Budd-Chiari syndrome.
Liver Biopsy
Biopsy of the liver in patients with this condition can show the following findings:
- Sinusoidal dilation due to stasis of blood flow
- Necrosis of hepatic cells in the centrilobular area
- Perisinusoidal fibrosis (mostly in the centrilobular region), which may evolve into cirrhosis
- Macro nodules in some cases
Biopsy is generally reserved for diagnostically unclear cases and is not routinely required.
Treatment of Budd-Chiari Syndrome
Treatment focus on:
- Alleviating the obstruction
- Prevention of the progression of the clot
- Limiting the progressive liver injury
- Prevention and management of complications
The goals of the treatment include:
- Relieving obstruction of occluded vessels
- Monitoring liver deterioration
- Correcting underlying conditions
The treatment approaches involve:
Anticoagulation
It is the first intervention on the absence of contraindications. Doctors initiate it with low molecular weight heparin and then switch to warfarin (continued lifelong). Patients with esophageal varices or other bleeding risks require careful management before starting therapy. While anticoagulation helps prevent clot progression, it does not usually reopen blocked veins on its own.
Thrombolysis
It is a treatment option within one month of clot development. It is considered highly successful if the clot involves either the IVC or the hepatic vein. Thrombolysis for chronic Budd-Chiari syndrome is contraindicated due to the risk of bleeding from complications of portal hypertension outweighing the benefit.
Angioplasty
Angioplasty with or without stent placement is used in acute and subacute cases, especially when there is a short narrowing or membrane in the hepatic veins or inferior vena cava. The stent helps keep the vessel open and maintain blood flow.
Surgical Shunts (TIPS)
Doctors place a transjugular intrahepatic portosystemic shunt (TIPS) in acute or subacute cases of Budd-Chiari syndrome that fail to respond to anticoagulation alone. This procedure helps reduce pressure in the liver and control complications of portal hypertension, and it may serve as a bridge to liver transplantation in severe cases.
Liver Transplantation
Liver transplantation is an option in patients who fail all therapies or those who have developed decompensated cirrhosis. Advanced age of the donor or recipient, a higher MELD score, and female transplant recipients can lead to poorer outcomes. Continuous anticoagulation can improve liver graft and patient survival rates.
Budd-Chiari syndrome Prognosis
Favorable prognostic factors in Budd-Chiari syndrome include younger age at diagnosis, absence or good control of ascites, preserved renal function, and a low Child-Pugh score. The Child-Pugh score is a clinical tool used to assess the severity of chronic liver disease based on blood tests and features such as ascites and hepatic encephalopathy. Patients who are diagnosed early and treated promptly generally have better outcomes.
Poor prognostic indicators include older age, persistent or refractory ascites, involvement of all hepatic veins or the portal vein, chronic presentation of the disease, and a high Child-Pugh score, reflecting more advanced liver dysfunction. The presence of renal impairment and progressive liver failure further worsens prognosis.
With modern stepwise management that includes anticoagulation, endovascular interventions, and liver transplantation when indicated, long-term survival now exceeds 70–80% in many patients.
Differential Diagnosis
Differential diagnoses of Budd-Chiari syndrome include the following conditions:
- Metastatic liver disease
- Right-sided heart failure or Congestive heart failure
- Fitz-Hugh-Curtis Syndrome (rare liver capsule inflammation associated with pelvic infection)
- Granulomatous liver disease (e.g., tuberculosis, sarcoidosis)
- Alcoholic liver disorder
- Infectious or Drug-induced hepatitis
- Cystic fibrosis
- Biliary atresia
- Inborn errors of metabolism (e.g., alpha-1 antitrypsin deficiency, neonatal hemochromatosis, congenital hepatic fibrosis, Niemann-Pick diseasetype C)
- Portal Vein thrombosis (obstruction of portal inflow rather than hepatic outflow)
These conditions should be considered when evaluating a patient with hepatomegaly, ascites, or abnormal liver tests, and imaging or laboratory findings do not clearly indicate Budd-Chiari syndrome.
Complications of Budd-Chiari Syndrome
Complications are mostly related to underlying conditions and the degree of liver failure. Untreated Budd-Chiari syndrome can lead to the following complications:
- Hepatic encephalopathy
- Portal hypertension
- Hepatorenal syndrome
- Variceal hemorrhage
- Hepatocellular carcinoma (long-standing liver congestion and cirrhosis can increase cancer risk)
- Bacterial peritonitis in the presence of ascites
Budd-Chiari Syndrome versus Portal Vein Thrombosis
Budd-Chiari syndrome involves obstruction of the hepatic veins or the inferior vena cava, leading to obstruction of hepatic outflow. On the other hand, portal vein thrombosis blocks inflow via the portal vein. Both of these conditions cause portal hypertension but differ in vascular sites, clinical presentation, and diagnostic imaging.
Key Differences
| Features | Budd-Chiari Syndrome | Portal Vein Thrombosis |
|---|---|---|
| Common causes | Myeloproliferative disorders and hypercoagulable thrombophilia | Malignancy, sepsis, cirrhosis, and prothrombotic state. |
| Sites | Hepatic veins or IVC outflow obstruction | Portal vein inflow obstruction |
| Acute symptoms | Severe abdominal painHepatomegalyAscitesJaundice | Often asymptomaticPainFeverVariceal bleeding (in chronic cases) |
| Onset | Rapid | Often gradual |
A Quick Review
In Budd-Chiari syndrome, the veins that carry blood away from the liver become blocked or narrowed. Inflammation and blood vessel obstructions are the main causes of this condition. Treatment options include blood thinners, minimally invasive procedures, and surgery, all of which focus on improving blood flow to the liver. Prompt treatment is essential. In severe cases, a liver transplant is the only option. Regular follow-up is essential to monitor the condition and lower the risk of developing complications.
References
[1] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[2] DeLeve, L. D., Valla, D. C., & Garcia‐Tsao, G. (2009). Vascular disorders of the liver.Hepatology,49(5), 1729-1764.
[3] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[4] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. In StatPearls [Internet]. StatPearls Publishing.
[5] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[6] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[7] Grus, T., Lambert, L., Grusová, G., Banerjee, R., & Burgetová, A. (2017). Budd-chiari syndrome.Prague Medical Report,118(2), 69-80.
[8] Menon, K. N., Shah, V., & Kamath, P. S. (2004). The Budd–Chiari syndrome.New England Journal of Medicine,350(6), 578-585.
[9] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[10] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[11] Dajti, E., Ravaioli, F., Colecchia, A., Marasco, G., Vestito, A., & Festi, D. (2019). Liver and spleen stiffness measurements for assessment of portal hypertension severity in patients with Budd Chiari syndrome.Canadian Journal of Gastroenterology and Hepatology,2019(1), 1673197.
[12] Hitawala, A. A., & Goosenberg, E. (2025). Budd-Chiari syndrome. InStatPearls [Internet]. StatPearls Publishing.
[13] Garcia-Pagán, J. C., & Valla, D. C. (2023). Primary budd–chiari syndrome.New England Journal of Medicine,388(14), 1307-1316.
[14] Koschmieder, S. (2020). How I manage thrombotic/thromboembolic complications in myeloproliferative neoplasms.Hämostaseologie,40(01), 047-053.
[15] Artru, F., Moschouri, E., & Denys, A. (2022). Direct intrahepatic portocaval shunt (DIPS) or transjugular transcaval intrahepatic portosystemic shunt (TTIPS) to treat complications of portal hypertension: indications, technique, and outcomes beyond Budd-Chiari syndrome.Clinics and research in hepatology and gastroenterology,46(4), 101858.
[16] Darwish Murad S, Plessier A, Hernandez-Guerra M, et al. Etiology, management, and outcome of the Budd-Chiari syndrome. Ann Intern Med. 2009;151(3):167-175.