
 is a life-threatening form of kidney failure that can only occur in patients with...){kind=link}

Hepatorenal Syndrome Kidneys Hepatorenal Syndrome (HRS) is a life-threatening form of kidney failure that can only occur in patients with advanced liver disease, most commonly cirrhosis with portal hypertension and ascites. It is a functional renal failure, meaning that although kidney function declines severely, the kidney structure remains intact. The kidneys stop functioning due to profound circulatory changes secondary to liver failure, particularly severe alterations in renal blood flow. This radical decrease in the blood flow to the kidney leads to a severe dual-organ failure involving both the liver and kidneys. HRS is a rapidly developing disease with a poor prognosis, and liver transplantation is the only solution. It develops in approximately 20–40% of patients with cirrhosis and ascites over the course of their disease.
What is Hepatorenal Syndrome?: Hepatorenal Syndrome Kidneys
Hepatorenal syndrome is a form of kidney failure that occurs specifically in patients with advanced liver disease. The mechanism is intense narrowing of the kidney blood vessels as a result of liver failure, which significantly decreases the glomerular filtration rate. Most importantly, the structure of the kidneys is normal. This is evidenced by:
- The transplantation of HRS kidneys into patients without liver disease, where they work normally, was successful.
- HRS patients undergoing liver transplant recover their renal function.
This confirms that the underlying cause of failure is circulatory and reversible, and can be corrected if liver function is improved.
The Causes of Hepatorenal Syndrome
Liver cirrhosis, including portal hypertension (elevated pressure in the blood vessels of the liver), is the most widespread underlying cause of HRS. This may be due to many conditions:
- Hepatitis B or C
- Liver disease caused by alcohol
- Metabolic dysfunction–associated steatotic liver disease (MASLD)
- Autoimmune liver diseases
- Bile duct disorders
- Hepatic metastatic malignancies
What Happens Inside the Body?
In cirrhosis, the liver becomes structurally altered, which makes it resistant to the blood flow. This, in its turn, discharges vasodilatory mediators that dilate the blood vessels within the intestinal area (splanchnic circulation). As a result, the effective arterial blood volume decreases, even though total body fluid may be increased.
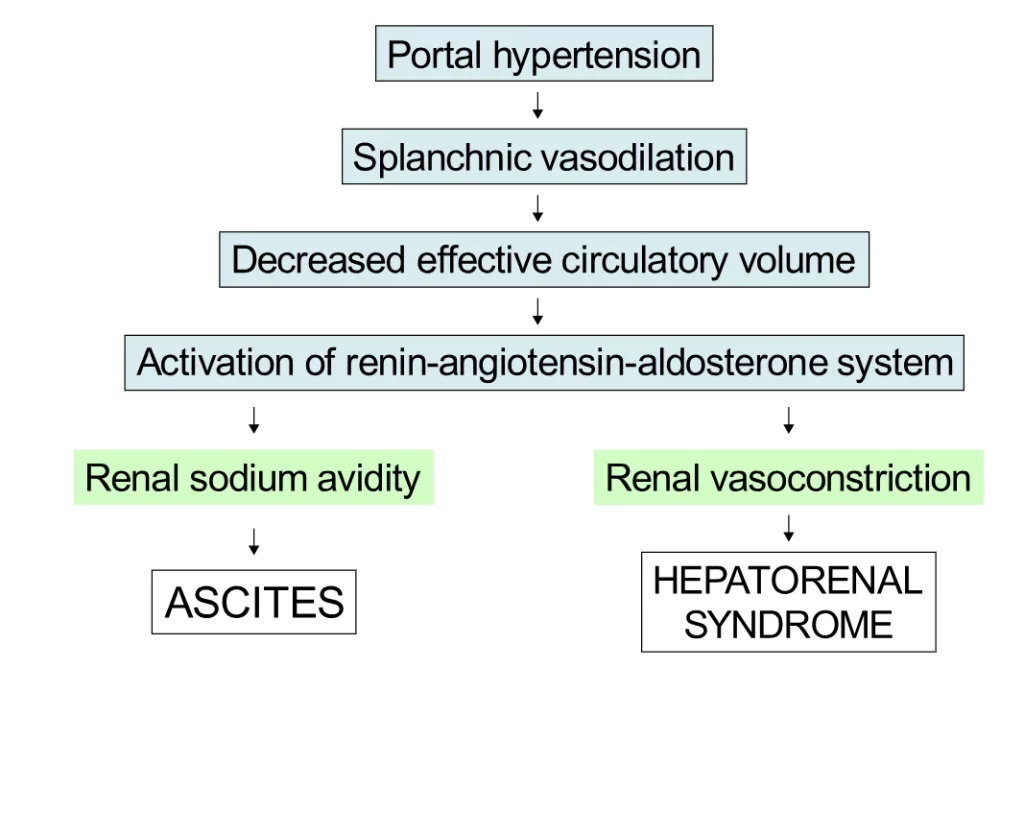
Schematic demonstrating the underfill theory, explaining how decreased effective blood volume contributes to both ascites and hepatorenal syndrome. Image credit: Samir aten.Wikipedia, CC BY 3.0.
The body interprets this as low blood pressure, and the compensatory mechanisms that the body takes up include:
- Activation of the renin–angiotensin–aldosterone system.
- Hypersensitivity of the sympathetic nervous system.
- Release of antidiuretic hormone.
These compensatory measures keep the blood pressure normal, leading to intense narrowing of blood vessels in the kidney. By so doing, the blood flow in the kidneys is severely curtailed, causing kidney failure.
Triggering Factors for HRS
Several events can precipitate the sudden onset of HRS in patients with advanced liver disease:
- Spontaneous bacterial peritonitis: One of the most common causes is the infection of ascitic fluid, and around a third of such individuals develop HRS.
- Large-volume paracentesis without albumin replacement.
- Gastrointestinal bleeding: Major blood loss.
- Aggressive diuretic therapy to get rid of an excess of fluid.
- Nephrotoxic drug use: Some drugs damage the kidneys, such as some antibiotics and painkillers.
Risk Factors
The risk of developing HRS increases in patients with:
- Low mean arterial pressure
- A low sodium level in the blood (Hyponatremia)
- High plasma renin and sympathetic activity
- Advanced cirrhosis with refractory ascites
- Urine sodium less than 5 mEq/L. However, it is important to note that urine sodium concentration and fractional excretion of sodium are no longer considered reliable diagnostic or predictive markers, particularly in patients receiving diuretics.
Hepatorenal Syndrome Types
HRS has been categorized according to the rate of decline in kidney function, and new terms are used to be specific.
HRS-AKI (Formerly Type 1)
- Acute progression: An increase in serum creatinine ≥0.3 mg/dL within 48 hours or ≥50% from baseline within 7 days, without requiring a minimum creatinine threshold.
- Low urine output: Patients have a lower urine output, which is usually below 500 mL/day.
- Acute triggers: In most cases, induced by infections, especially bacterial peritonitis.
- Poor prognosis: Median survival in the absence of treatment is about two weeks, with very few cases surviving longer than 10 weeks.

Comprehensive infographic outlining the diagnostic criteria for HRS-AKI and HRS-NAKI, highlighting creatinine changes, eGFR thresholds, and cirrhosis with ascites.
HRS-NAKI (Formerly Type 2)
- Moderate impairment: The functioning of the kidneys degrades at a slower pace, with moderately elevated but stable creatinine levels
- Related to refractory ascites: This primary clinical presentation is the non-response to diuretic fluid build-up.
- Better prognosis: Median survival is around 3-6 months, with the number being still much lower than that of cirrhosis patients without kidney dysfunction.
- Nature: Can evolve into HRS-AKI.
Hepatorenal Syndrome Symptoms
HRS symptoms may be challenging to identify since they may be similar to the symptoms of severe liver disease. To get it early, it is important to notice any change in your health. Pay attention to the small shifts in your mood.
The Early Stage:
At the start, there is an increase in:
- Weakness and fatigue
- Loss of appetite
- Nausea
- General malaise
These feelings are shared with liver disease, making them easy to rule out, and thus, HRS is frequently diagnosed later.
Progressive Symptoms
As soon as the malfunction of the kidneys starts to be more marked, the symptoms become more evident, in particular, with reference to the urine and to the aggravation of the liver-related problems:
Urinary Changes:
Alterations in urination are a huge red flag.
- The production of low volumes of dark, concentrated urine
- Less frequent urination
- Urination can almost be stalled in extreme cases
Liver Disease Manifestations:
- Yellowness of skin and eyes (jaundice) is more enhanced
- More ascitic fluid in the abdomen
- Swelling in the legs and feet (edema)
- Signs of hepatic encephalopathy
- Easier bruising or bleeding
The Possible Complications
HRS may cause other severe issues, like hazardous imbalances in blood salts (electrolytes), extreme fluid retention, and an increased susceptibility to infections, any of which will cause you to feel even worse.
Hepatorenal Syndrome Diagnosis
Hepatorenal syndrome (HRS) is a challenging diagnosis to make, with no one confirmatory test. It is characterized by fulfilling certain clinical criteria and eliminating other possible causes of kidney failure.

Digital illustration highlighting liver–kidney involvement in hepatorenal syndrome.
Diagnostic Criteria (HRS-AKI)
- There should be cirrhosis with ascites.
- Acute kidney injury (AKI): increase in creatinine ≥0.3mg/dL in 48hours or 50% compared to baseline in 7 days.
- No improvement after diuretic withdrawal and albumin administration (1 g/kg/day, max 100 g/day) for 2 days
- Absence of shock
- None of the nephrotoxic drugs in recent history or an indication of structural kidney damage
Laboratory Tests
Several laboratory investigations help in diagnosis:
Blood Tests:
- Serum creatinine levels (elevated)
- Blood urea nitrogen (elevated)
- Electrolytes showing low sodium
- Abnormal Liver function tests
Urine Tests:
- Low sodium (<10 mEq/L), high osmolality, low protein, and absence of hematuria or casts.
New Biomarkers
New Biomarkers used to differentiate between HRS and damage in kidney tissue are:
- The most promising is Neutrophil Gelatinase-Associated Lipocalin or NGAL: low in HRS, high in acute tubular necrosis
- Cystatin C
- Kidney Injury Molecule-1 (KIM-1)
- Liver-type Fatty Acid Binding Protein (L-FABP)
- Cell cycle arrest biomarkers (TIMP-2 and IGFBP7)
These markers are adjunctive tools and not yet universally available or standardized.
Imaging Studies
While not diagnostic on their own, imaging studies help exclude other causes:
- Renal ultrasound: HRS has a normal kidney size and structure as compared to chronic kidney disease.
- Doppler ultrasound: Could be used to measure the renal resistive index, which is usually increased in HRS.
- Shear wave elastography: New technology that has the potential to aid in measuring kidney rigidity and prognosis.
Management of Hepatorenal Syndrome
Therapy of HRS is aimed at reversing the impairment of kidney functionality, controlling complications, and, eventually, providing conclusive treatment using liver transplantation. The treatment has greatly changed over the last years with improved knowledge and newer drugs.
Medical Management: First-Line Therapy
Vasoconstrictor Drugs in Association with Albumin
The basis of HRS treatment is medications that constrict the intestinal region blood vessels but increase blood volume:
Terlipressin plus Albumin (First-line option)
- One of the synthetic vasopressin analogs that induces selective vasoconstriction is terlipressin.
- Accepted by the FDA according to the CONFIRM trial.
- Dosing: Initial dose of 1 mg every 4–6 hours, titrated as needed
- Combined with albumin: 1 g/kg body weight on day 1, followed by 20-40 g daily
- Response rate: 32-40% get reversal of HRS
Alternative Vasoconstrictors: Where terlipressin is not available, alternative Vasoconstrictors are used. - Norepinephrine: Continuous infusion, similar efficacy, as shown in some studies, as terlipressin.
- Midodrine combined with Octreotide: Not as effective as terlipressin.
- Close supervision needs an ICU environment to administer and monitor patients.
Only 40-50% of patients receiving vasoconstrictor therapy achieve an overall response, which is a serum creatinine level that returns to ≤1.5 mg/dL. The survival of these responders is much higher, whereas non-responders need other strategies, and some first responders are recurrent.
Renal Replacement Therapy (Dialysis)
In cases of medical treatment failure, dialysis can be done to treat serious complications such as uremia, electrolyte imbalance, or fluid overload, or serve as a bridge to liver transplant. There are modalities of traditional hemodialysis or dedicated liver support systems, such as the Molecular Adsorbent Recirculation System or MARS. Nevertheless, without transplantation mortality is high, and only a small proportion (10–15%) of patients regain kidney function on chronic dialysis.
Liver Transplantation: The Ultimate Cure
The ultimate treatment of HRS is liver transplantation, which is the cure of the underlying liver failure. After an isolated liver transplant, about 69-70 percent of the patients undergo kidney recovery, usually in days to weeks, and survival is long-term, as with other recipients of liver transplants who do not have HRS.
Nevertheless, there is also a risk that some of them will develop chronic kidney disease. Immediate transplantation gives good results, particularly in progressing Type 1 HRS. During waiting time, patients undergo medical treatment to help their kidneys work properly, and their renal dysfunction is automatically noted in the MELD scoring system in order to rank above other patients in the waiting line.
Combined Liver-Kidney Transplantation
Combined liver-kidney transplantation can also be discussed in the case of kidney dysfunction, which lasts more than 4–6 weeks, and the glomerular filtration rate remains low, dialysis is required constantly, and structural kidney impairment occurs. Nevertheless, this is not a simple choice, since in certain instances, hepatorenal syndrome may resolve following liver transplantation alone, and it is therefore not easy to estimate which patients really need both organs.
Prevention of Hepatorenal Syndrome
Preventive strategies play a critical role in reducing the incidence of hepatorenal syndrome and improving outcomes in patients with advanced cirrhosis, particularly those with ascites and spontaneous bacterial peritonitis (SBP).¹¹
In patients with SBP, intravenous albumin administration (1.5 g/kg on day 1 and 1 g/kg on day 3) has been shown to significantly reduce the risk of renal impairment and HRS by approximately 40%, as well as decrease mortality.
Additional preventive measures include:
- Avoid Nephrotoxic drugs
- Careful use of diuretics
- The replacement of albumin after large-volume paracentesis
- Timely management of infections.
- Maintain blood pressure
- Frequent check of kidney functions
Hepatorenal Syndrome Prognosis
Hepatorenal syndrome has a very poor prognosis, but contemporary therapy has shown better results. Type 1 HRS is a quickly fatal disease with a median survival of only two weeks without treatment, whereas Type 2 HRS has a median survival of 3-6 months.
40-50 percent of patients respond well to medical treatment. The responders have a much improved survival of more than six months, whereas the non-responders have an equal prognosis to the untreated patients. Despite treatment, mortality during the 90 days is high (45-51).
The only opportunity to have a definite cure is provided by liver transplantation, which has a significant positive impact on the prognosis. HRS patients undergoing transplantation and recovering their kidney functions show far superior results compared to patients whose kidney functions never recover.
Hepatorenal Syndrome Life Expectancy
The knowledge of the life expectancy of HRS patients, their families, and health care providers is essential in making decisions relating to treatment and care planning.
By Type and Treatment Life Expectancy.
By Type and Treatment Life Expectancy
| HRS Type | Without Treatment | With Medical Treatment | With Liver Transplant |
|---|---|---|---|
| Type 1 HRS (HRS-AKI) | 2 weeks median; <10 weeks maximum | 1-3 months median (if responds); <1 month (if no response) | 3-5+ years (70%+ survive 1 year) |
| Type 2 HRS (HRS-NAKI) | 3-6 months median; ~30% survive 1 year | 6-12 months median (with treatment) | 3-5+ years (similar to Type 1 post-transplant) |
Conclusion
Hepatorenal Syndrome (HRS) is a severe severe but potentially reversible complication of advanced liver disease. Although its prognosis is poor, its diagnosis and treatment using modern methods can be of great help.
Definitive cure is only a liver transplant, which in many cases results in the recovery of the kidney. In the case of a number of patients, medical therapy is an important step to transplantation. The management requires early detection and communication between the hepatology and nephrology teams.
Hope of recovery and long survival is possible with timely intervention and all-time care and particularly the candidates of transplantation.
References
[1] Iwatsuki S, Popovtzer MM, Corman JL, et al. Recovery from “hepatorenal syndrome” after orthotopic liver transplantation.N Engl J Med. 1973;289(22):1155-1159. doi:10.1056/NEJM197311292892202
[2] Koppel, M. H., Coburn, J. W., Mims, M. M., Goldstein, H., Boyle, J. D., & Rubini, M. E. (1969).Transplantation of cadaver kidneys from patients with hepatorenal syndrome. New England Journal of Medicine, 280(25), 1367–1371. https://doi.org/10.1056/NEJM196906192802502
[3] Gines, P., Schrier, R. W. (2009).Renal failure in cirrhosis. New England Journal of Medicine, 361(13), 1279–1290. https://doi.org/10.1056/NEJMra0809139
[4] Simonetto DA, Gines P, Kamath PS. Hepatorenal syndrome: pathophysiology, diagnosis, and management.BMJ. 2020;370:m2687. doi:10.1136/bmj.m2687
[5] Duailibe JBB, Viau CM, Saffi J, Fernandes SA, Porawski M. Hepatorenal syndrome: Current concepts and future perspectives.World J Nephrol. 2024;13(3):95627. doi:10.5527/wjn.v13.i3.95627
[6] Emre, S., & Bucuvalas, J. C. (2025).Hepatorenal syndrome causing acute kidney injury (HRS-AKI). In EMCrit IBCC CME. Retrieved from https://cmefix.emcrit.org/ibcc/hrs
[7] Angeli P, Garcia-Tsao G, Nadim MK, Parikh CR. News in pathophysiology, definition and classification of hepatorenal syndrome: a step beyond the International Club of Ascites (ICA) consensus document.J Hepatol. 2019;71(4):811-822. doi:10.1016/j.jhep.2019.07.002
[8] Biggins SW, Angeli P, Garcia-Tsao G, et al. Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and Hepatorenal Syndrome: 2021 Practice Guidance by the American Association for the Study of Liver Diseases.Hepatology. 2021;74(2):1014-1048. doi:10.1002/hep.31884
[9] Belcher JM, Sanyal AJ, Peixoto AJ, et al. Kidney biomarkers and differential diagnosis of patients with cirrhosis and acute kidney injury.Hepatology. 2014;60(2):622-632. doi:10.1002/hep.26980
[10] Wong F, Pappas SC, Curry MP, et al. Terlipressin plus albumin for the treatment of type 1 hepatorenal syndrome.N Engl J Med. 2021;384(9):818-828. doi:10.1056/NEJMoa2008290
[11] Wong TC, Fung JY, Pang HH, et al. Analysis of survival benefits of living versus deceased donor liver transplant in high model for end-stage liver disease and hepatorenal syndrome.Hepatology. 2021;73(6):2441-2454. doi:10.1002/hep.31584
[12] Lee JP, Kwon HY, Park JI, et al. Clinical outcomes of patients with hepatorenal syndrome after living donor liver transplantation.Liver Transpl. 2012;18(10):1237-1244. doi:10.1002/lt.23493
[13] Ruiz R, Barri YM, Jennings LW, et al. Hepatorenal syndrome: a proposal for kidney after liver transplantation (KALT).Liver Transpl. 2007;13(6):838-843. doi:10.1002/lt.21149
[14] Sort P, Navasa M, Arroyo V, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis.N Engl J Med. 1999;341(6):403-409. doi:10.1056/NEJM199908053410603
[15] Peluso L, Savi M, Coppalini G, et al. Management of hepatorenal syndrome and treatment-related adverse events.Clin Med Insights Gastroenterol. 2024;17. doi:10.1177/11795514241256431
[16] Bass L, Kapoor S, Rochwerg B, et al. Early diagnosis and timely terlipressin in hepatorenal syndrome improves projected outcomes and lowers cost.Clin Gastroenterol Hepatol. 2024. doi:10.1016/j.cgh.2024.06.021