
{kind=link}

Dermatofibroma It Worry You may notice a small, firm bump on your skin. It has been there for months. It does not hurt much, but it is not going anywhere either. If this sounds familiar, you may be looking at a dermatofibroma. It is one of the most common, harmless skin growths out there, and yet it causes a fair amount of worry simply because most people have never heard of it.
What Is a Dermatofibroma?: Dermatofibroma It Worry
Dermatofibroma is a benign, common, cutaneous soft-tissue lesion that presents as a firm nodule arising from the dermis, sometimes extending into the subcutaneous tissue. It is also called fibrous histiocytoma, and the name refers to the morphologic appearance of the cell populations that constitute these lesions. It is, in other words, a small, hard lump composed of fibrous tissue located in the dermis (and sometimes extending into deeper layers of the skin).
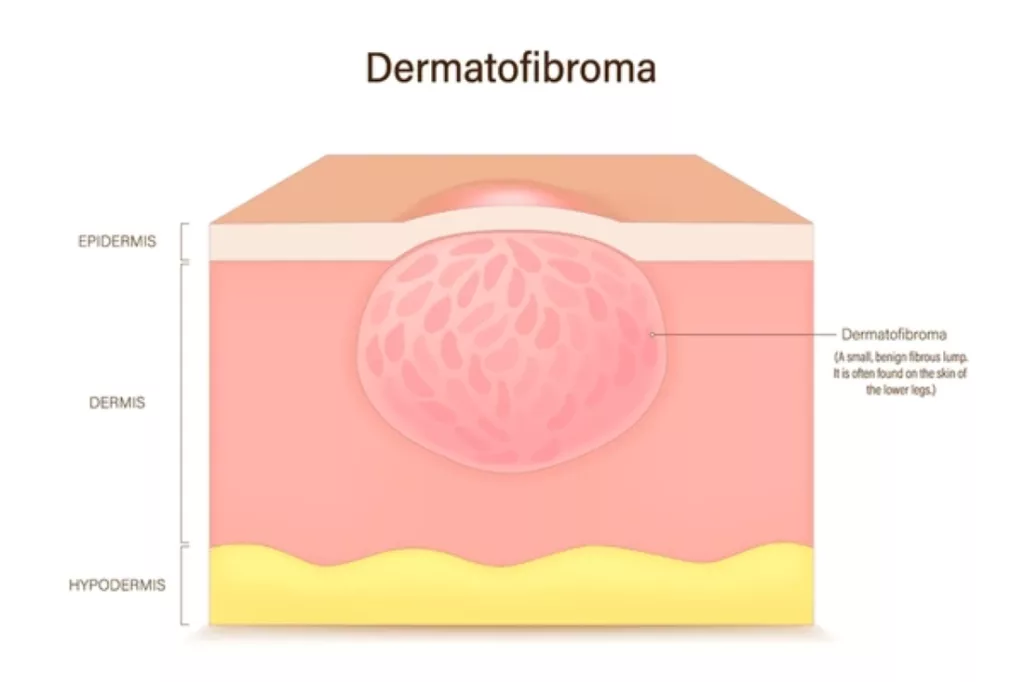
Medical vector illustration showing dermatofibroma, a benign fibrous skin tumor.
A dermatofibroma is the typical overgrowth of the fibrous tissue located in the deepest of the two primary skin layers, the dermis. It is not cancerous and does not transform into cancer. This is likely the most critical fact to be aware of. Although it is strange to look at and even scares others at times, it does no harm.
These dermal lesions are usually distributed clinically on the extremities and are comparatively small, usually not more than 1 cm. Dermatofibromas are common in all age groups, although they are more common in people between 20 and 50, and mostly in women.
What Does a Dermatofibroma Look Like?
The images of dermatofibroma tend to represent a tiny, round, elevated, and easily confused bump with a mole. Dermatofibromas are benign tumors in the skin that are typically small, with a diameter of between 0.5 and 1.5 centimeters. They may be of any color, though in light skin, they are usually pink or light brown, and in dark skin, dark brown or black. The color can be pinker or darker in case an individual irritates them, say, during shaving. They are firm and hard to touch, and therefore, people say that they feel as though they are a small stone that is there below the skin or above the skin.
A dermatofibroma can be clinically suspected by a very helpful test, which is the dimple sign or pinch test. The pinch test involves pinching the sides of the skin lesion between the thumb and the finger. When the lesion is dimpled or indented, it is probably a dermatofibroma. When a regular mole is pinched, it remains raised. A dermatofibroma is anchored; thus, it draws in because it is embedded in the deeper layers of skin. This is one of the observations that a doctor considers when a physical examination is conducted.

A doctor performing the pinch test on a dermatofibroma, which dimples when squeezed from the sides.
The surface of the skin is smooth and, in some cases, scaly. The color of the skin is skin-colored, pink/red, cream/white, or brown. Once it has grown initially, the bump is usually maintained at a constant size without any further increase in size.
Where Does a Dermatofibroma Most Often Appear?
A dermatofibroma is a benign nodule that is a common fibrous nodule typically present on the skin of the lower legs. Dermatofibroma of the leg is by far the most common presentation, and that is why many individuals only notice it after shaving first. However, they may be found on the upper arms, the back, and other regions as well.
These nodules are prevalent in adults but not in children. They may be in the form of pink, gray, red, and brown.
Most people have just one. Dermatofibromas can occur in more than one person, and these may predispose them to develop more. Several forms are likely to develop in case of impaired immunity, including autoimmune disease, systemic lupus erythematosus, HIV, or leukemia.
What Causes a Dermatofibroma?
Here, the situation becomes slightly less clear. It is still unclear what causes dermatofibroma. Nonetheless, they usually appear following a minor dermal injury, including a prick attack by a thorn or an insect bite.
Conventionally, a response to trauma, like insect bites, was considered the cause of dermatofibromas. But its cause is not known very well. Others believe that they are benign neoplasms, as opposed to being reactive.
So what causes dermatofibroma? To conclude, it has not been reduced to a single answer in science. What we do know is that:
- They are usually associated with insect bites, minor skin trauma, ingrown hairs, and shaving-related cuts.
- Approximately one out of five patients with a dermatofibroma experienced some form of injury or wound at the location where the tumor grows. The dermatofibroma sometimes develops without any known cause.
- Dermatofibromas are not considered hereditary.
- Women have twice as many dermatofibromas as men.
The body, in a way, sometimes reacts to even a small skin irritation by overgrowth of fibrous tissue, and it is this overgrowth that is what we call dermatofibroma.
Symptoms: How Does It Feel?
Dermatofibromas do not generally produce any symptoms; however, pain, tenderness, or itchiness can occur. Most individuals simply pay attention to them due to the bump they see, but not because it is painful.
That said, a dermatofibroma on the leg may become a recurring problem. When shaving the skin over the legs, it may result in bleeding.
The summary of typical symptoms includes:
- A firm, compact bump that is not bigger than 1.5 cm.
- Depending on the skin colour, it may be pink, brown, or dark.
- In some cases, mild itching or tenderness.
- A depression of the skin is formed when it is pinched.
- Pain on bumping, touching, or catching clothes.
How Is It Diagnosed?
Diagnosis is usually clinical and based on physical examination, although other lesions may mimic its appearance.
Dermatofibroma tends to be clinically easy to diagnose with the help of dermoscopy. The typical dermoscopic appearance shows a central white scar-like area with a peripheral pigment network.
In other instances, further research is required. Diagnostic excision or skin biopsy is performed in case of an atypical appearance, such as recent enlargement, ulceration, or asymmetrical structures and colors on the dermoscopy.
Most doctors are very serious about unusual cases in order to rule out a condition known as dermatofibrosarcoma protuberans (DFSP). It is important to distinguish between benign dermatofibromas and more developed and malignant neoplasms, which can be similar in appearance. DFSP is a low- to intermediate-grade, locally aggressive tumor that can resemble a dermatofibroma clinically.
This is the reason why it is always worth visiting the doctor with any emerging or transforming skin growth, regardless of whether it appears to be harmless or not.
Dermatofibroma Removal: Do You Actually Need It?
Here is the reassuring part. Usually, there is no need to treat the lesion unless it is symptomatic. Dentomyofibromas usually persist and rarely regress spontaneously. The nodules remain permanent unless they are removed. However, since they are benign, some individuals just prefer to leave them alone.
Others may want to have their dermatofibromas excised when the dermatofibroma is unattractive, occupies an inconvenient site such as a shaving nick or is agitated by clothing or painful or itchy.
Before proceeding with removal, it is worth remembering that patients who want to have the lesion excised on cosmetic grounds must be told that the scar that can be left may be even more prominent than the original lesion, especially on the lower extremities. That is, the cure may even be more conspicuous than the issue itself, at least initially.
Dermatofibroma Removal Options
In case removal is selected, a number of methods exist. Here is a clear comparison:
| Treatment Method | How It Works | Best For | Key Consideration |
|---|---|---|---|
| Surgical Excision | The lesion is cut out under local anesthesia | Complete, permanent removal | May leave a more visible scar |
| Cryotherapy | The lesion is frozen by using liquid nitrogen. | Smaller, superficial growths | May need multiple sessions; risk of pigment changes |
| Laser Therapy | Specific energy dissolves fibrous tissue. | Shallow lesions; numerous growths. | Less invasive; results may vary |
| Shave Removal | The top part of the lesion is shaved off | Cosmetic reduction | Higher chance of recurrence |
| Punch Removal | Circular machine cuts the growth. | Moderate-depth lesions | Small scar; stitches may be needed |
The commonly used removal options are discussed in detail below:
Surgery
Surgical excision is considered the most definitive approach. Total excision, which is accompanied by the subcutaneous fat, is the best procedure in case the lesions are not cosmetically acceptable, especially symptomatic, or when there is uncertainty regarding diagnosis. It has been demonstrated that a 3-mm margin is adequate to remove typical dermatofibromas completely.
Cryotherapy
An alternative to surgery that is popular is cryotherapy. Direct application of liquid nitrogen to the lesion will lead to freezing of the cells and subsequent sloughing. It is a fast office procedure that does not involve stitches, and most of the patients are typically able to resume activities shortly after undergoing the procedure. Nevertheless, cryotherapy can induce long-term and short-lived alterations in skin color, especially in the darker-skinned population.
Laser Therapy
Laser therapy can be used to achieve a highly targeted treatment and thereby reduce the destruction of adjacent tissue. It is quite applicable to a person who has multiple growths or prefers not to be operated on at all.
Surgical removals can lead to bleeding, infection, and scarring. These are mostly minor and can be managed effectively with appropriate care, but need to be discussed with your doctor before occurrence.
When Should You See a Doctor?
A majority of dermatofibromas are completely benign and will never bring any serious trouble. Yet, there are cases when it is significant to seek a professional opinion. You should see a doctor if:
- The bump is growing rapidly or changing in shape
- The colour is changing or becoming irregular
- It begins to bleed without getting wounded
- You do not know whether it is a dermatofibroma or not
- It is causing persistent pain or itching
Although dermatofibromas are harmless, an individual is advised to inform a physician of any emerging skin formation, particularly when it is varying in its size, shape, or color, or shows an abnormal arrangement. They are also supposed to report any growth that bleeds, causes pain, itches, or grows at an alarming rate. In other instances, these growths can point to other related, though severe, skin disorders.
A Final Word
Dermatofibroma is one of those skin conditions that sounds more alarming than it actually is. It is a very tiny and solid, benign nodule that is usually located along the lower leg, and it remains in the same place throughout life without being harmful. It may itch sometimes or be stuck on a razor, but it does not run the risk of becoming cancerous, and it hardly needs any medical attention.
Knowledge of what a dermatofibroma is, its causes, identification in photographs, and possible times of consideration of dermatofibroma removal leaves you in a far better situation to make a rational, relaxed response to the health of your skin.
In case of any suspicion, a visit to a dermatologist is never the wrong choice. They are able to verify the diagnosis in a short period of time, calm you down, and talk you through the possibilities, in case removal is something you decide to do at some point in your life.
References
[1] Han TY, Chang HS, Lee JH, Lee WM, Son SJ. A clinical and histopathological study of 122 cases of dermatofibroma (benign fibrous histiocytoma).Ann Dermatol.2011;23(2):185–192.
[2] Zaballos P, Puig S, Llambrich A, Malvehy J. Dermoscopy of dermatofibromas: a prospective morphological study of 412 cases.Arch Dermatol.2008;144(1):75–83.
[3] Alves JV, Matos DM, Barreiros HF, Bartolo EA. Variants of dermatofibroma — a histopathological study.An Bras Dermatol.2014;89(3):472–477.
[4] Bergman R, Friedman-Birnbaum R, Hazaz B, Cohen I, Munichor M, Lichtig C. An immunohistochemical study of the origin of dermatofibromas.Am J Dermatopathol.1988;10(4):296–305.
[5] Bedir R, Güçer H, Şehitoğlu İ, Yurdakul C, Üstün H. Dermatofibroma: clinical and dermoscopic features in 65 cases.North Clin Istanb.2016;3(1):11–16.
[6] Zaballos P, Llambrich A, Puig S, Malvehy J. Dermoscopic findings in pigmented purpuric dermatoses.Br J Dermatol.2004;150(6):1112–1116.
[7] Colome-Grimmer MI, Evans HL. Metastasizing cellular dermatofibroma: a report of two cases.Am J Surg Pathol.1996;20(11):1361–1367.
[8] Karsai S, Roos S, Hammes S, Raulin C. Pulsed dye laser: what’s new in non-vascular lesions?J Eur Acad Dermatol Venereol.2007;21(7):877–890.
[9] Kuflik EG. Cryosurgery for skin cancer: 30-year experience and cure rates.Dermatol Surg.2004;30(2):297–300.
[10] Horenstein MG, Prieto VG, Shea CR. Atypical (“pseudosarcomatous”) focal dermal hypoplasia: a case report and review of the literature.J Cutan Pathol.2000;27(6):288–292.