
{kind=link}

Kissing Disease Symptoms Kissing Disease, the term used for Infectious Mononucleosis, gets its name from transmission through saliva, most commonly via close contact such as kissing. It is also called “mono” for short, and can be referred to as glandular fever. It is a widespread viral infection caused by the Epstein-Barr Virus (EBV) that primarily affects teenagers and young adults. If you catch the disease, you can expect general symptoms of fever, tiredness, or sore throat that usually subside within a few weeks and only require symptomatic treatment.
How prevalent is Kissing Disease?: Kissing Disease Symptoms
In the US, the incidence of kissing disease is 500 in every 100,000 people. This means that 1 in every 200 people will have a symptomatic infection. Worldwide, 95% of adults have immunity against the EBV virus, but many do not show symptoms due to becoming seropositive during childhood.
Who is at risk?
Although it can occur at any age, the mode of transmission via saliva (rather than casual airborne spread) makes it common among young adults and people living in shared quarters. Teenagers (15-19) and young adults (up to 24 years) are more likely to ‘catch’ mono due to casual socialising, kissing, and sharing personal items between peers. Similarly, individuals living in shared quarters, such as dorms, hostels, or slums, have a higher chance of developing mono due to the possibility of close contact with an infected person.

Friends are enjoying a social gathering, sharing drinks and laughter. These situations can facilitate the transmission of infectious mononucleosis.
How do you get mononucleosis?
Infectious Mononucleosis is mainly caused by the Epstein-Barr Virus (EBV), which is a member of the herpes family. Other viruses, such as Cytomegalovirus (CMV), may cause mono as well. These viruses are highly contagious, and transmission from an affected individual to a healthy individual occurs through bodily fluids, primarily saliva. This can happen in several ways:
- Sharing contaminated items, such as utensils, drinks, and toothbrushes, is the primary cause of transmission.
- Similarly, kissing involves close contact with saliva and may also involve its transfer. This is where the disease gets its name from, but it’s not limited to kissing only.
- Coughing or sneezing releases salivary droplets into the air. These droplets can contaminate any surfaces or food and aid in transmission. However, transmission through respiratory droplets or contaminated surfaces is less common compared to direct saliva contact.
- In rare cases, blood transfusion or organ transplantation from an infected individual can result in the development of symptoms.
Pathogenesis of EBV
When the Epstein-Barr Virus enters the body of an individual through the transfer of contaminated saliva, it settles and replicates in the epithelial cells of the mouth and throat, i.e., the oropharynx. After replicating, it infects the B lymphocytes (white blood cells) present in the lymph tissues of the oropharynx. This starts a cascade of immune reactions and the activation of T-lymphocytes. As the lymphocytes proliferate in the lymph tissue, they cause swelling of the lymph nodes and a sore throat. After the initial infection resolves, EBV establishes lifelong latency in B lymphocytes. Periodic viral shedding can occur in saliva without causing symptoms. However, the patient will not have any symptoms, since they have already developed immunity against the disease.
What are the signs and symptoms of mono?
Symptoms typically appear four to six weeks after infection and can range from mild to severe. Since it is a viral infection, the symptoms overlap with other viral infections and can present as:
- Fever: High temperature, lasts for one to two weeks, and is the most common symptom.
- Pharyngitis: Sore and painful throat, difficulty swallowing due to infection of the epithelial cells in the oropharynx.
- Lymphadenopathy: The lymph nodes in the neck are swollen, since EBV proliferates in the lymph tissues of the head and neck. Swollen lymph nodes in the back of your neck are characteristic of mono.
- Swollen tonsils: They appear red and swollen, with pus-like discharge, showing white or yellow exudate.
- Extreme fatigue accompanied by headaches, body aches, and loss of appetite.
- Mono Rash: A maculopapular rash may occur, especially after the use of aminopenicillin antibiotics (such as amoxicillin or ampicillin), and is not a true drug allergy.
- Hepatosplenomegaly: Enlarged spleen and liver due to an activated immune system. An enlarged spleen occurs in about 50% people by the second week.
- Bilateral periorbital oedema (Hoagland sign): A characteristic S-shaped swelling of the upper eyelids. It is one of the early signs, before other symptoms occur (after about 5 days of onset), and is characteristic of mono. The swelling resolves spontaneously.
[Image: A diagram of a human body with labelled symptoms of kissing disease (infectious mononucleosis). ]
Diagram showing the common symptoms of kissing disease (infectious mononucleosis), including fatigue, fever, sore throat, swollen lymph nodes, and an enlarged spleen. Image credit: Mikael Häggström.Main symptoms of infectious mononucleosisviaWikimedia Commons.
What are the complications of Infectious Mononucleosis?
Infectious mononucleosis is a self-limiting illness and resolves on its own. It rarely ever develops any complications, and they mostly occur in immunocompromised individuals. They include:
- Airway obstruction: Excessive swelling of the lymph nodes and tonsils can lead to a constricted airway and difficulty breathing.
- Blood disorders such as hemolytic anaemia, thrombocytopenia (low platelet levels), pancytopenia (reduction of all red blood cells, white blood cells, and platelets), or hemolytic uremic syndrome.
- Cardiac symptoms, including inflammation of the heart tissues (myocarditis, pericarditis) and arrhythmias, may occur.
- Splenic rupture: If the spleen is enlarged in the patient and they indulge in strenuous activities or sports, the spleen can rupture. This usually occurs in the first three weeks of the onset of the disease. It requires immediate hospitalisation and even surgery.
- Liver inflammation can lead to hepatitis or jaundice.
- Skin involvement in the form of erythema multiforme, antibiotic-associated rash, and oral hairy leukoplakia are rare complications of mono.
- Eye symptoms may include inflammation of the different layers of the eye (episcleritis, uveitis), leading to photophobia and sensitivity to light.
- Nervous System involvement includes meningitis, encephalitis, and Guillain-Barré syndrome.
- EBV is also associated with certain malignancies such asBurkitt lymphoma, Hodgkin lymphoma, and nasopharyngeal carcinoma, particularly in specific populations or immunocompromised individuals.
How long does mono last?
The prognosis of Kissing Disease is very favourable, and the infection resolves on its own. The acute symptoms (fever and sore throat) subside by the second week of onset, but fatigue can persist for up to six months. Although EBV can remain present in saliva for several months, the risk of transmission is highest during the acute phase of illness.
How to Diagnose Kissing Disease?
History
The physician will ask you about your symptoms, their duration, and their severity. They might also enquire if youve been in contact with an infected person with similar symptoms.
Initial Examination
The physician will record your fever and examine your throat to check for redness, swollen tonsils, and/or any pus coming out from the tonsils. They will also perform a head and neck examination to check for swollen and tender lymph nodes.
Diagnostic Investigations4Mayo Clinic. Mononucleosis – diagnosis and treatment [Internet]. mayoclinic.org. 2018.:
- The most common diagnostic test is the Monospot test and is also known as the “Hetrophile antibody test.” A blood sample is taken via the prick of a finger and tested for heterophile antibodies that are produced by EBV. The sensitivity of this test is about 70-90%, because it can give false negatives for children or in the early stage of the disease, where the antibodies have not formed yet. It can give false positives due to HIV, CMV, Hepatitis, or other diseases that produce heterophile antibodies.
- Complete Blood Count (CBC) represents high white blood cells and increased lymphocytes. Liver function tests may also show mild elevation of transaminases.
- The EBV-Specific Antibody Test is done when the monospot test is negative, but mono is highly suspected. The test detects antibodies such as VCA-IgM, VCA-IgG, and EBV nuclear antigen (EBNA).
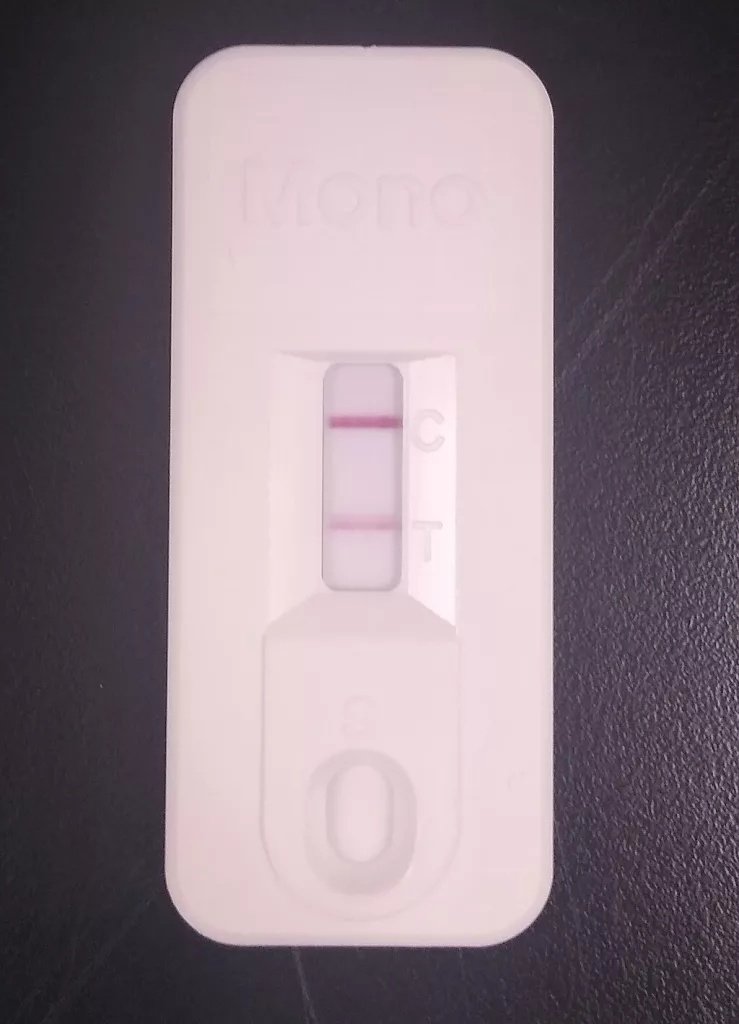
A rapid immunochromatographic test used to detect heterophile antibodies in a blood sample, helping doctors diagnose infectious mononucleosis. Image source:Wikimedia Commons,Immunochromatographic rapid test for infectious mononucleosis, heterophile antibody testlicensed under CC-BY 4.0
Hoagland’s Criteria Infectious Mononucleosis
Since Infectious Mononucleosis mimics other viral diseases, and the monospot test can be false negative, definitive diagnosis is done according to Hoagland’s criteria. The criteria consist of:
- Presence of clinical triad: Fever, pharyngitis, lymphadenopathy.
- Laboratory blood tests showing more than 50% lymphocytes of the total white blood cells, out of which there are more than 10% are atypical lymphocytes.
While Hoagland’s criteria are useful, modern diagnosis relies on a combination of clinical findings and serological testing. Although this criterion is specific to mono, not all cases will meet all requirements, and exceptions may occur.
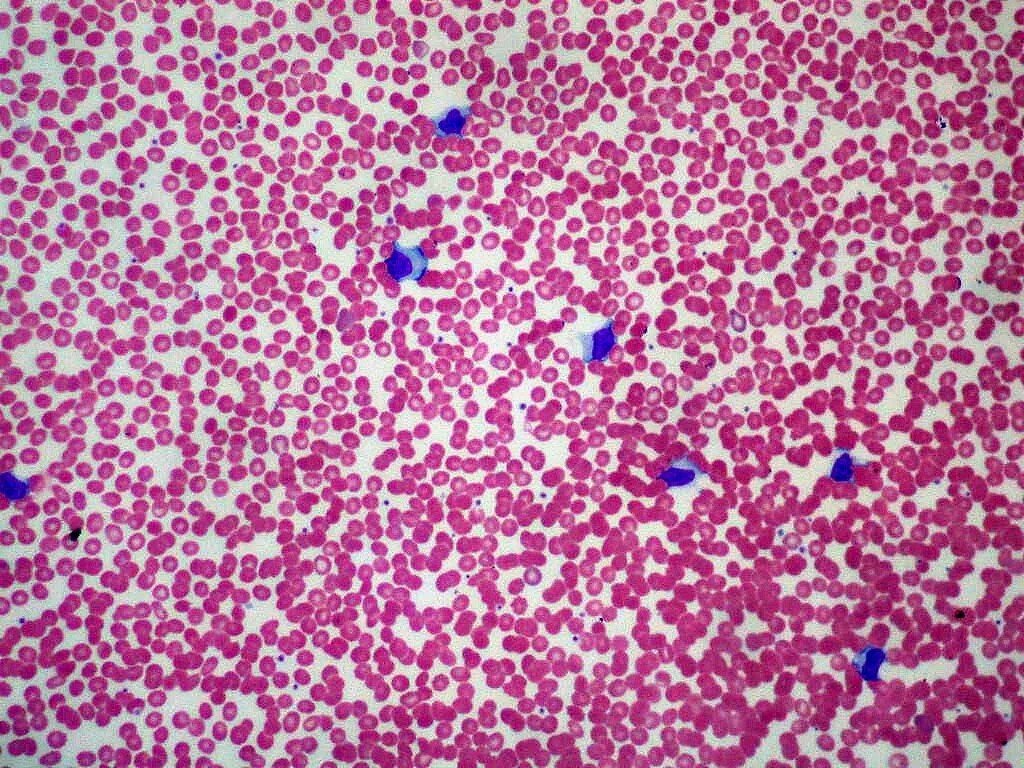
Peripheral blood smear from a patient with infectious mononucleosis showing an increased number of lymphocytes, a typical laboratory finding in the kissing disease. Image credit: Ed Uthman, MD. “Infectious Mononucleosis – peripheral blood smear showing lymphocytosis.” Available viaWikimedia Commons. Licensed under CC BY-SA 2.0.
Differential Diagnosis of mono
Since the symptoms of kissing disease are general and overlap with other viral infections, it can easily be confused with other diseases. Viruses such as CMV, HIV, Herpes family, Toxoplasmosis, and Hepatitis B are included in its differentials. Mono can be confirmed via the monospot test, as that will be negative for CMV, HIV, and Toxoplasmosis. It can also be confused with streptococcal pharyngitis, which presents with similar sore throat and fever, but typically lacks the profound fatigue and generalised lymphadenopathy of mono.
Treatment of Infectious Mononucleosis
Being a viral disease, Infectious Mononucleosis has no specific treatment, but requires palliative care. Medications such as antibiotics or antivirals are not effective in treating mono. Your doctor might suggest the following:
- Rest is key to letting your body fight the infection. Drink lots of fluids to keep yourself hydrated, and eat nutritious food to fuel your body. Avoid strenuous activities or social gatherings until your symptoms subside. The more rest you get, the sooner you will recover and feel better.
- Fever and body aches can be managed by nonsteroidal anti-inflammatory drugs (NSAIDs) (e.g., Advil, Brufen) or acetaminophen (Panadol).
- Sore throat management is achieved through symptomatic treatment of pain, cough, and other symptoms. Painkillers, throat lozenges, and warm saline gargles help soothe the throat.
- Antiviral medication such as Acyclovir or Valacyclovir may be prescribed, but they are not that effective in treating the disease in healthy patients. It may be used as an adjunct in severe complications and systemic involvement.
- In cases of airway obstruction due to swollen tonsils, corticosteroids (such as prednisone or dexamethasone) may be administered to reduce inflammation and swelling.
Take Away
If you know someone who has recently developed Infectious Mononucleosis, it is best to avoid sharing drinks, utensils, or closed spaces with that individual to prevent catching the disease. If you do catch mono, the symptoms can feel overwhelming due to intense fatigue, high fever, and sore throat, but the disease is self-limiting and resolves by itself. Over-the-counter painkillers are helpful as supportive care for symptomatic relief.
Recognising the symptoms early can also help prevent unnecessary antibiotic use and reduce the spread of infection through shared drinks, utensils, or close contact. Since the virus can remain dormant in the body after recovery, most individuals develop long-lasting immunity and rarely experience symptomatic reinfection.
Overall, awareness of the disease, its transmission, and appropriate recovery measures helps ensure a smooth recovery while minimising complications and transmission to others.
References
[1] Dakota TH PharmD, BCPS Assistant Professor of Pharmacy Practice South Dakota State University College of Pharmacy Clinical Pharmacist, Sanford USD Medical Center Sioux Falls, South Dakota Kaitlyn Jude, PharmD Candidate South Dakota State University College of Pharmacy Brookings, South Dakota Brittney Meyer, PharmD Assistant Professor of Pharmacy Practice South Dakota State University College of Pharmacy Brookings, South. Management Options for Infectious Mononucleosis [Internet].
[2] Thorley-Lawson DA, Hawkins JB, Tracy SI, Shapiro M. The pathogenesis of Epstein–Barr virus persistent infection. Current Opinion in Virology. 2013 Jun;3(3):227–32.
[3] Otsuki T, Ishizuka K, Hirose M, Ie K. Hoagland sign in infectious mononucleosis. BMJ Case Reports [Internet]. 2022 Nov;15(11):e252839.
[4] Mayo Clinic. Mononucleosis – diagnosis and treatment [Internet]. mayoclinic.org. 2018.
[5] Stuempfig ND, Seroy J. Monospot Test [Internet]. PubMed. Treasure Island (FL): StatPearls Publishing; 2020.
[6] Differential Diagnoses | Infectious Mononucleosis (IM) [Internet]
[7] De Paor M, O’Brien K, Fahey T, Smith SM. Antiviral agents for infectious mononucleosis (glandular fever). Cochrane Database of Systematic Reviews. 2016 Dec 8;
[8] Gomes K, Goldman RD. Corticosteroids for infectious mononucleosis. Canadian Family Physician. 2023 Feb;69(2):101–2.
[9] Rezk E, Nofal YH, Hamzeh A, Aboujaib MF, AlKheder MA, Al Hammad MF. Steroids for symptom control in infectious mononucleosis. Cochrane Database of Systematic Reviews. 2015 Nov 8;