
{kind=link}

An ‘empty sella’ is a radiological sign seen on CT or MRI. The sella is not actually empty but is filled with CSF that has pushed the gland flat against the floor of the cavity, giving it the appearance of an empty space on imaging. Empty sella refers to a radiological finding, while empty sella syndrome is diagnosed when this finding is associated with clinical or hormonal abnormalities.
Historically, it was thought that there were no clinical consequences of an empty sella. However, now we know that in many people with empty sella, there can be neurological and endocrine consequences of varying degrees. The condition is more common than most people realize: around 35% of the general population shows an empty sella on imaging.[1]
What is Sella Turcica?
Sella turcica, Latin for “Turkish saddle”, is a depression in the sphenoid bone at the base of the skull. It cradles and protects the pituitary gland, so it is also called the pituitary fossa or the hypophyseal fossa.
The top of the sella is covered by a dural (dura mater, part of the meninges) fold called the diaphragma sellae, a thin membrane with a small central opening that allows the pituitary stalk to pass through.[2]

The pituitary gland sits within the sella turcica at the base of the skull. In empty sella syndrome, cerebrospinal fluid compresses the gland against the sellar floor. (Image credit: NIDDK, NIH viaWikipedia Commonsand licensed Public domain)
The pituitary gland is pea-sized, roughly 1cm in diameter, and located directly below the hypothalamus. It is often called the ‘master gland’ of the endocrine system, because the hormones it releases regulate hormone production in other glands. This is why clinical consequences in empty sella syndrome are so broad. Fatigue, irregular periods, infertility, low libido, weight changes, and temperature intolerance all seem unrelated but trace back to pituitary hormones.
Empty Sella vs Empty Sella Syndrome
Empty sella syndrome is the radiological finding of an empty sella that is also accompanied by clinical consequences. The subarachnoid space (fluid-filled space around the brain) herniates (pushes) through the diaphragma sellae into the pituitary fossa. As a result, CSF accumulates inside the sella turcica.[3]
The CSF pushes the pituitary against the sellar floor, compressing and flattening it. The stalk (infundibulum) also becomes stretched. On imaging, the sella appears partially or completely filled with CSF rather than pituitary tissue. In most cases, the pituitary continues to function normally despite being compressed.
The word “syndrome” only applies when symptoms are present, and that is in around 42% of empty sella cases. An empty sella without symptoms is just a radiological finding.
What Causes Empty Sella Syndrome?
An empty sella can be either primary or secondary, depending on the underlying cause.
Primary Empty Sella (PES):
We label the condition as primary when there is no identifiable prior injury or disease to explain the finding. In these cases, the cause is anatomical: the diaphragma sellae has a congenital weakness, it’s either too thin or incomplete.
Over time, even a normal or slightly elevated intracranial pressure (ICP) can push the arachnoid membrane through. This herniated sac fills with CSF and expands within the bony sella, and the pituitary gets progressively compressed.
Primary empty sella is often associated with some risk factors:
- Obesity and hypertension can raise ICP
- It is 4-5 times more common in women
- Middle age (40-60)
- Multiple pregnancies since the pituitary is known to enlarge during each pregnancy and then involutes post-lactation, but still leaves space behind
- Idiopathic intracranial hypertension (IIH) is a major driver because of chronically raised ICP; up to 70-94% of IIH patients have empty sella on MRI[4]
Despite the size, pituitary function is preserved in the majority. Studies show an estimated 15-52% of people with PES develop hypopituitarism, i.e., deficiency in one or more pituitary hormones.[5]
Secondary Empty Sella (SES):
In secondary cases, the pituitary gland has been damaged, destroyed, or reduced in size by a specific event, which leaves the bony sella larger relative to what remains of the gland. The causes include:
- Surgical removal or debulking of a pituitary tumor or even spontaneous regression
- Radiotherapy to the gland or sellar region
- Hemorrhage or infarction into the pituitary gland
- Sheehan’s syndrome, which is postpartum pituitary necrosis following massive haemorrhage at delivery, is associated with a drop in blood pressure
- Autoimmune inflammation of the pituitary gland, most common in women close to delivery
- A traumatic brain injury
- Infection, sarcoidosis, or congenital pituitary hypoplasia
Hormonal deficits are far more common in secondary empty sella than in the primary form. Adrenal insufficiency, which is potentially life-threatening, is found in >50% of SES cases.
Partial vs Complete Empty Sella Syndrome
An empty sella is labeled partial or complete based on the radiological emptiness. If more than 50% of the sella is occupied by CSF and pituitary thickness is ≤2 mm on MRI, it is complete empty sella. If less than 50% of the sella appears occupied by CSF and pituitary thickness is ≥3 mm, it is a partial empty sella.
That said, studies do not show any correlation between pituitary volume on MRI and hormone levels. Some patients with partial findings have significant hormone deficits, while some with complete findings have completely normal function.[6]
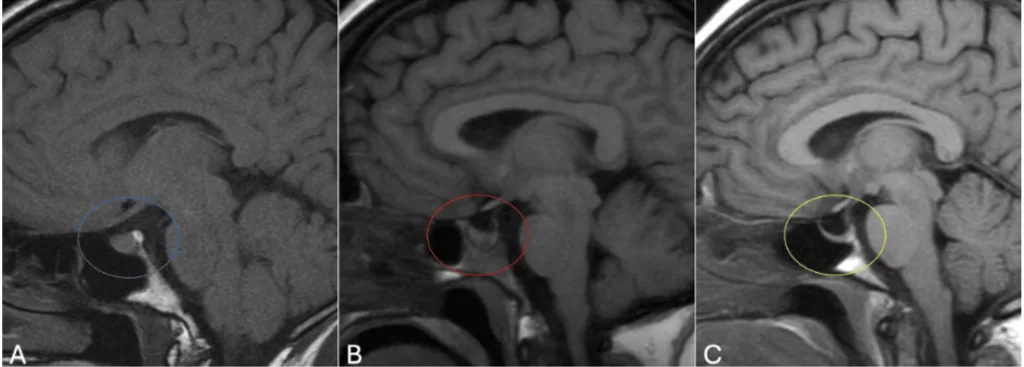
Sagittal MRI scans showing varying degrees of sellar emptiness. Panel A shows a normal sella with the pituitary, panel B a partial empty sella, and panel C a completely empty sella with the pituitary gland flattened to a thin rim at the sellar floor. (Image Courtesy: Rice-Canetto T E, Carroll P, Reier L, et al. (December 18, 2024) Asymptomatic Empty Sella: A Literature Review and Suggestions for Evaluation in Clinical Practice. Cureus 16(12): e75965. Available fromCureusand licensed under CC by 4.0)
Symptoms of Empty Sella Syndrome
The symptoms patients present with in empty sella syndrome can either be related to the underlying causes or be a consequence of hormonal dysfunction. Many symptoms are non-specific, so patients end up being investigated for a while before the pituitary connection is made.
Neurological Symptoms:
The most common symptom is a chronic headache because of raised intracranial pressure. Other consequences can be pulsatile tinnitus, dizziness, and syncope. Less commonly, we see mood disturbances and cognitive difficulties, which might be because of raised ICP or a tumor.
Visual Symptoms:
These are also usually because of raised intracranial pressure instead of the empty sella itself. When the optic chiasm prolapses into the sella, visual field defects may be seen. The classic finding is a bitemporal hemianopia where vision is lost in the outer halves of both the left and right visual fields.
Raised ICP can also cause double vision (diplopia) by pressing on the cranial nerves III, IV, and VI. Other than this, patients complain of blurred vision or general visual acuity loss. Another sign found on fundoscopy is papilloedema: swelling of the optic disc.
CSF Rhinorrhea:
In extreme cases, chronic CSF pulsation pressure can even erode the bony sellar floor. The CSF then starts leaking through into the sphenoid sinus and then into the nasal passages, presenting as clear watery nasal discharge, which can get mistaken for a runny nose. CSF rhinorrhea is rare, but it carries a huge risk of ascending meningitis.[7]

The pituitary gland regulates multiple hormonal axes. In empty sella syndrome, compression of the gland can disrupt one or more of these, producing a wide and apparently unrelated range of symptoms. (Image Courtesy: Bian Y, Hahn H, and Uhmann A (2023). The hidden hedgehog of the pituitary: hedgehog signaling in development, adulthood, and disease of the hypothalamic-pituitary axis. Front. Endocrinol. 14:1219018. Available fromFrontiersand licensed under CC by 4.0)
Hormonal Manifestations:
Hormonal manifestations are because of hypopituitarism. In primary ESS, approximately 34% patients develop hypopituitarism, compared to about 64% in secondary ESS.[8] The severity depends on which axis is affected.
- Hypogonadotropic hypogonadism is the most common in PES. Low LH and FSH result in low estrogen and testosterone, which can present as irregular or absent periods (oligomenorrhoea/amenorrhoea), infertility, low libido, erectile dysfunction, and loss of secondary sexual characteristics.
- Hypothyroidism, because of low TSH, causes fatigue, weight gain, cold intolerance, constipation, dry skin, and even cognitive slowing
- Adrenal insufficiency is the most common consequence of secondary ESS. Low ACTH from the pituitary results in low cortisol, which manifests as fatigue, weight loss, nausea, hypotension, salt craving, and an inability to start a stress response, which is potentially life-threatening.
- Growth hormone deficiency can cause fatigue, central obesity (abdominal fat), reduced muscle mass, and poor bone density.
- Hyperprolactinemia is seen in around 5% of cases because compression of the pituitary stalk disrupts dopamine delivery from the hypothalamus. Low dopamine means prolactin is not inhibited, and it manifests as galactorrhoea, menstrual irregularities, and low libido.
- ADH deficiency causes central diabetes insipidus, with excessive thirst and urination.
The posterior pituitary is usually spared in most primary ESS cases, and total disruption of anterior pituitary function is present in approximately 12% of all ESS cases.
How to Lose Weight with Empty Sella Syndrome?
Growth hormone deficiency, hypogonadism, and hypothyroidism can all individually and collectively cause weight gain. GHD causes central adiposity, hypothyroidism slows down the basal metabolic rate, and hypogonadism affects fat distribution. The result is that normal weight loss strategies fail to make a difference.
If someone with ESS is struggling to lose weight, the first step has to be getting the hormones tested and treated. If deficient, hormone replacement to restore thyroid hormones, sex steroids, and growth hormone can normalize metabolism, making it possible to lose weight by using standard weight management strategies like a calorie-deficit diet and exercise. Exercise improves insulin sensitivity and helps manage comorbidities (hypertension, metabolic syndrome) commonly associated with ESS.
If IIH is present, weight loss itself is a treatment because it will reduce intracranial pressure. Studies show that a sustained loss of even 5-10% body weight can significantly reduce ICP.[9] Bariatric surgery is effective for IIH but evidence for ESS is limited. It should be considered in severely obese patients with IIH-driven ESS.
Diagnosis of Empty Sella Syndrome
An empty sella is often an incidental finding on CT or MRI being done for a headache, trauma, or routine checkup. A formal diagnosis of empty sella syndrome requires a combination of the radiological findings, clinical symptoms, and hormonal assessment.
Full assessment includes:
- Detailed patient history about prior pituitary surgeries, radiotherapy, head trauma, postpartum hemorrhage, and medication history.
- BMI and blood pressure measurement for major risk factors (obesity, hypertension)
- Brain MRI is the gold standard for confirming and characterising the empty sella
- Neurological examination
- Ophthalmic assessment: visual acuity, visual field testing (perimetry), fundoscopy
- Full pituitary hormone panel through blood tests
- If IIH is suspected, a lumbar puncture is done to measure the opening pressure (>25 cmH2O with normal CSF composition confirms IIH)
- In case of CSF rhinorrhea, high-resolution CT cisternography or MRI cisternography to identify the leak site
Radiology for Empty Sella Syndrome
MRI is the gold standard imaging modality for diagnosis. A CT can identify an enlarged sella as well, but lacks the soft tissue resolution to assess the gland itself. MRI findings also help characterize the ESS as partial or complete.
Classic MRI findings of empty sella are:
- An enlarged sella turcica filled with CSF
- The pituitary gland is compressed into a thin semilunar rim along the floor
- The pituitary stalk is deviated or stretched. ESS shows the ‘central stalk sign’: the infundibulum remains midline and descends to the sellar floor, instead of cystic lesions where the stalk is displaced laterally.[10]
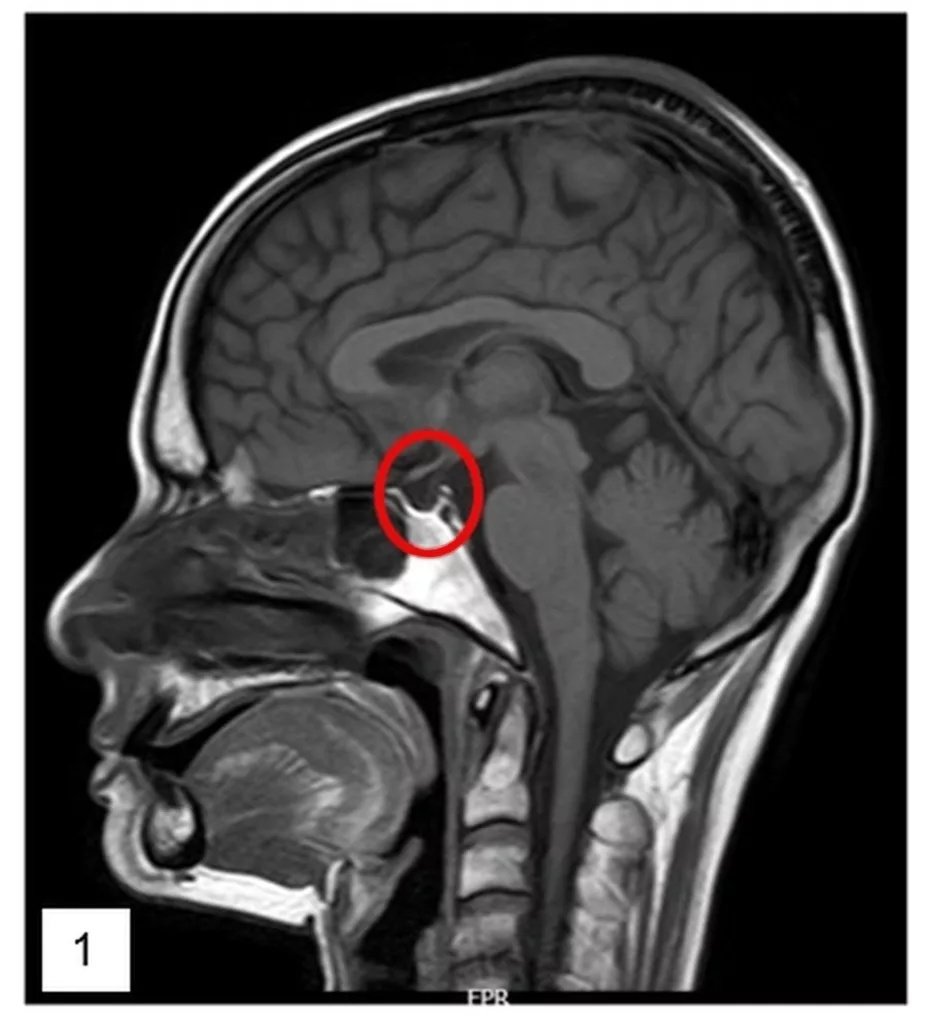
Sagittal MRI scan showing an empty sella. The cavity is filled with CSF, and the pituitary is flattened, visible only as a thin rim along the wall of the cavity. (Image Courtesy: Ahamed M A A, Shetty S, Hegde S, et al. (September 08, 2022) The Emptiness Within: A Case of Empty Sella Syndrome. Cureus 14(9): e28941. Available from Cureus and licensed under CC BY 4.0.
At the same time, it is important to look for signs of raised ICP, like flattening of the posterior globe of the eye, distension of the perioptic subarachnoid space, or an elongation of the optic nerves.
Blood Tests for Empty Sella Syndrome
Even if there are no neurological or visual symptoms or a raised ICP, it is important to assess the function of the pituitary gland. After imaging diagnoses the structural findings and confirms ESS, blood tests assess the functional consequences. For this, all five pituitary axes need to be assessed.
- Thyroid axis: TSH, free T4 (low fT4 in addition to low/normal TSH)
- Adrenal axis: ACTH levels; morning serum cortisol is important; if borderline, we proceed to dynamic testing, e.g., short Synacthen test (SST) or insulin tolerance test (ITT)
- Gonadal axis: LH, FSH, oestradiol in females, testosterone in males, prolactin in both
- Growth hormone/IGF-1 axis: IGF-1 is the screening test; if it is low or borderline, dynamic testing with ITT or glucagon stimulation test is done to confirm GHD.[11]
- Posterior Pituitary: ADH assessment (serum, urine osmolality, serum sodium)
- Other than these, routine blood tests, including a full blood count and metabolic panel
How is Empty Sella Syndrome Treated?
If there is just the radiological finding, no symptom or hormonal deficit, no treatment is needed at all. If there is a hormonal deficit, hormone replacement therapy is paramount to replace the defect: Levothyroxine for hypothyroidism, recombinant growth hormone therapy, or dopamine agonists for hyperprolactinemia in case of stalk compression.
Raised intracranial pressure, if present, has to be treated separately and on priority. In obese patients, the first line is weight loss, along with:
- Acetazolamide 250-1000mg/day to reduce CSF production
- Diuretics
- Repeated lumbar puncture for immediate relief
- If the patient reports progressive visual loss despite treatment, the optic nerve sheath is decompressed by making a small opening in the sheath to relieve pressure.
In extreme cases with CSF rhinorrhea, medicines aren’t enough; the eroded floor has to be repaired via surgery: endoscopic closure and packing of the sella to raise the pituitary gland back up.[12]
Takeaway
In most cases, ESS is not life-threatening. An incidental empty sella has an excellent prognosis and doesn’t usually progress to hormone dysfunction. However, if hormone deficits are left untreated, the patient is most likely to have increased cardiovascular morbidity and mortality. The most dangerous complication is adrenal insufficiency in secondary ESS.
Once an empty sella finding is made on radiology, all patients should have at least one complete pituitary panel assessment so that those with a hormonal dysfunction can be monitored and treated. If one hormonal axis is affected, it is recommended that all others be assessed as well. Compared to adults, children warrant closer monitoring because GHD can affect their growth.
References
[1] Rice-Canetto, T. E., Carroll, P., Reier, L., & Siddiqi, J. (2024). Asymptomatic Empty Sella: A Literature Review and Suggestions for Evaluation in Clinical Practice. Cureus, 16(12), e75965.
[2] Maingard J, Diaphragma sellae. Reference article, Radiopaedia.org
[3] Ucciferro P, Anastasopoulou C. Empty Sella Syndrome. [Updated 2023 Oct 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan.
[4] Sarrami, A. H., Bass, D. I., Rutman, A. M., Alexander, M. D., Aksakal, M., Zhu, C., Levitt, M. R., & Mossa-Basha, M. (2022). Idiopathic intracranial hypertension imaging approaches and the implications in patient management. The British journal of radiology, 95(1136), 20220136.
[5] Carosi G, Brunetti A, Mangone A, Baldelli R, Tresoldi A, Del Sindaco G, Lavezzi E, Sala E, Mungari R, Fatti LM, Galazzi E, Ferrante E, Indirli R, Biamonte E, Arosio M, Cozzi R, Lania A, Mazziotti G and Mantovani G (2022) A Multicenter Cohort Study in Patients With Primary Empty Sella: Hormonal and Neuroradiological Features Over a Long Follow-Up. Front. Endocrinol. 13:925378.
[6] Kałuża, B., Furmanek, M., Domański, J., Żuk-Łapan, A., Babula, E., Poprawa, I., Landowska, M., Jarząbek, K., Popczyńska, J., Filipowicz, P., Wielgolewska, M., Walecki, J., & Franek, E. (2025). The Influence of Pituitary Morphology on the Occurrence of Hormonal Disorders in Patients with Empty Sella or Partial Empty Sella. Biomedicines, 13(4), 762.
[7] Daudia, A., Biswas, D., & Jones, N. S. (2007). Risk of meningitis with cerebrospinal fluid rhinorrhea. The Annals of otology, rhinology, and laryngology, 116(12), 902–905.
[8] Steckel, L., Gizewski, E. R., & Kaser, S. (2025). Pituitary function in patients with primary and secondary empty sella. Frontiers in endocrinology, 16, 1632824.
[9] Mollan, S. P., Mitchell, J. L., Yiangou, A., Ottridge, R. S., Alimajstorovic, Z., Cartwright, D. M., Hickman, S. J., Markey, K. A., Singhal, R., Tahrani, A. A., Frew, E., Brock, K., & Sinclair, A. J. (2022). Association of Amount of Weight Lost After Bariatric Surgery With Intracranial Pressure in Women With Idiopathic Intracranial Hypertension. Neurology, 99(11), e1090–e1099.
[10] Gaillard F, Niknejad M, Celery stalk sign (anterior cruciate ligament). Reference article, Radiopaedia.org
[11] Fatani T. H. (2023). Diagnostic Value of IGF-1 in Growth Hormone-Deficient Children: Is a Second Growth Hormone Stimulation Test Necessary?. Journal of the Endocrine Society, 7(4), bvad018.
[12] Araujo Filho, B. C., Butugan, O., Pádua, F. G., & Voegels, R. L. (2005). Endoscopic repair of CSF rhinorrhea: experience of 44 cases. Brazilian journal of otorhinolaryngology, 71(4), 472–476.