
 is a vascular disease characterized by narrowing of the left common iliac vein (LCIV), which...){kind=link}

May Thurner Syndrome May-Thurner syndrome (MTS) is a vascular disease characterized by narrowing of the left common iliac vein (LCIV), which runs between the right common iliac artery (RCIA) and the lower part of the spine. The arteries are the blood vessels that carry blood from the heart to the body. The veins are the tubes that return blood from the body to the heart. When the vein is compressed between the artery and the spine, it can cause highly variable symptoms. The right common iliac artery supplies oxygenated blood to the right lower limb, while the iliac veins return deoxygenated blood from the lower body to the heart. MTS interrupts typical blood flow through your legs.
Most people with LCIV compression have no symptoms. Sometimes MTS may cause symptoms and even lead to the formation of blood clots, also known as deep vein thrombosis (DVT). Hence, the condition can occur with or without DVT. The condition is named after the doctors who first described it in the 1950s.
Causes of May-Thurner Syndrome
MTS is primarily an anatomical issue, where the right common iliac artery (RCIA) compresses the LCIV against the spine. This compression arises from the normal anatomical crossover of blood vessels in the pelvis. Pulsations from the artery damage the vein’s inner lining, forming the fibrous spurs that narrow the vein further. There are several risk factors of the condition, which include:
- Female gender (Women are five times more likely to develop MTS than men, especially those who are in the postpartum stage, pregnant, or who use oral contraceptives.
- People aged 18-50.
Other contributors include:
- Scoliosis
- Dehydration
- Multiple Pregnancies
- Family history of venous issues
Pathophysiology of May-Thurner Syndrome
The pathophysiology is not completely known. However, it is believed that chronic pulsations from the artery induce shear stress and endothelial injury in the vein, triggering the deposition of collagen and elastin. This forms intraluminal fibrous spurs or bands that narrow the vein lumen. The resulting stenosis impairs venous return and promotes blood stasis, which may increase the risk of DVT. Many cases stay asymptomatic due to collateral veins, but acute leg swelling can signal thrombosis.
Signs and Symptoms of May-Thurner Syndrome
Most patients do not present with symptoms; however, progression to significant narrowing or complete closure of the vein can occur, leading to swelling of the left leg. Some other symptoms include:
- Changes in skin color
- Hardening of the skin
- Thinning of the skin
- Development of the sores on the lower part of the leg (Venous stasis)
The swelling usually involves the entire affected leg. It is noticeably larger than the opposite leg. MTS patients also experience venous claudication (thigh or leg pain and tightness that occur with exercise and resolve with rest or leg elevation).
The symptoms may occur gradually or suddenly. They can come and go, or worsen, throughout the day. This usually happens after prolonged standing or sitting. The symptoms usually affect the left leg or pelvis, but right-sided and both-sided symptoms of MTS have also been reported.
Diagnosis of May-Thurner Syndrome
The Diagnosis of MTS involves a comprehensive physical examination and imaging.
Physical Examination
The physical examination includes a complete set of vital signs, a thorough cardiopulmonary examination, and assessment of both lower legs.
Imaging
The initial test to evaluate leg swelling is a venous duplex ultrasound (Doppler ultrasound).
Doppler Ultrasound
This is a non-invasive and readily available technique. It is operator-dependent and can measure venous flow, categorize reflux volume, measure vessel diameter, and assess for stenosis and obstruction.
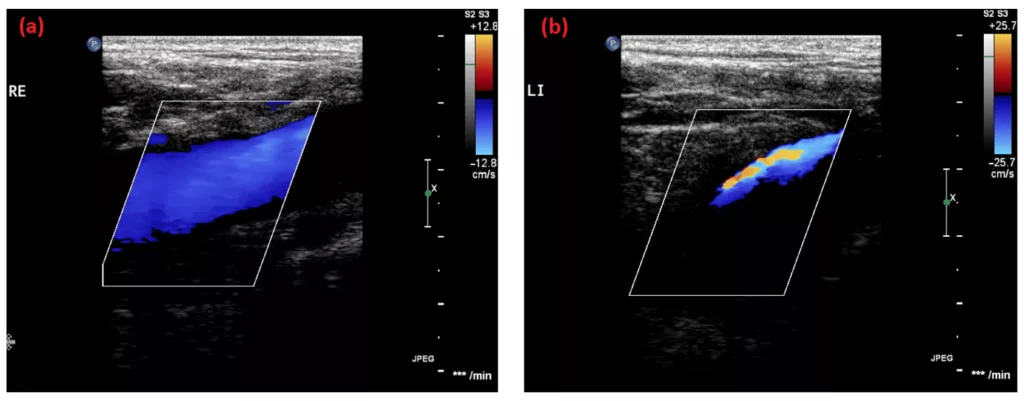
Ultrasound images of the (a) right and (b) left femoral vein of the 19-year-old brother. Turbulence and a decrease in vein diameter in the left vein compared to the right side indicate a venous compression syndrome. Image Courtesy: Familiar Disposition of May–Thurner Syndrome—A Case Series by Nowak et al, 2024, doi.org/10.3390/life14020221, available via: https://www.mdpi.com/2075-1729/14/2/221, CC BY 4.0.
CT Venography
It has 95% sensitivity and specificity for detecting iliac vein compression. CT venograpgy can visualize the stenosis, collaterals, and DVT. It can exclude other causes of iliac vein compression, such as hematoma, malignancy, and lymphadenopathy. CT angiography must be avoided in pregnancy in people with renal insufficiency.
MR Venography
MR venography is comparable to CT, but it offers better delineation of structures and is acceptable during pregnancy. An isolated MR venography is insufficient to diagnose MTS effectively. However, MR venography is more expensive and less readily available than CT and Doppler venography.
Intravascular Ultrasonography
It has a sensitivity greater than 98% for iliac compression. Intravascular Ultrasonography can characterize the location and severity of stenosis, thrombus, and fibrosis. It is capable of precise measurements. It is considered the gold standard for confirming clinically significant iliac vein compression, especially during endovascular procedures. It is the only imaging modality that can identify and quantify subtle changes in the vessel. Intravascular ultrasonography is an invasive technique and is not widely available. It cannot provide information about the surrounding anatomical structures.
Management and Treatment of May-Thurner Syndrome
The management of the MTS depends on symptoms and the presence of thrombosis. The primary goal of treatment is to restore normal blood flow through the compressed common iliac vein. Treatment also focuses on removing any clots that may have formed due to narrowing. It is generally reserved for patients with symptoms (most commonly those with new DVT).
Conservative Management
For mild symptoms without clots, use compression stockings and leg elevation. You need to change your lifestyle and avoid prolonged immobility. Additionally, anticoagulation prevents clots in higher-risk patients. Delaying initiation of anticoagulation is associated with an increased risk of life-threatening pulmonary embolism (PE).
AngioplastyAngioplasty
The healthcare provider inserts a catheter with a balloon tip into the left iliac vein. The balloon inflates or opens the vein when it is in the correct position. The provider then places a small mesh tube, called a stent, in the vein to keep it open and then removes the balloon. Angioplasty avoids compressing the artery. This is currently the first-line definitive treatment for symptomatic MTS with significant compression or DVT.
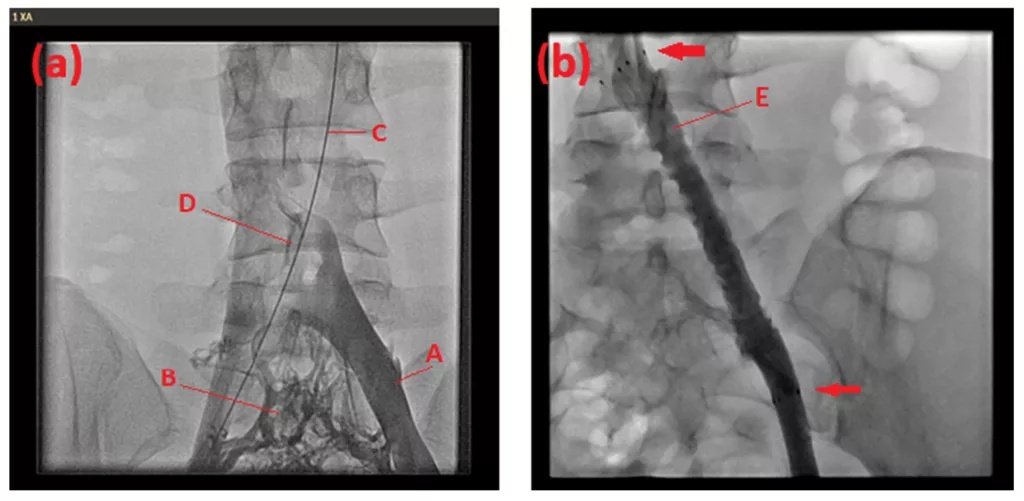
Venography of the 16-year-old patient (a) before and (b) after stent implantation. Left common iliac vein (A). Venous collaterals (B). Guide wire placed in the right iliac artery and aorta (C). Filling defect of contrast medium indicating the venous stenosis located at the arterial overcrossing (D). Left common iliac vein after balloon dilatation and stent implantation (E). Proximal and distal stent end (arrows). Image Courtesy: Familiar Disposition of May–Thurner Syndrome—A Case Series by Nowak et al, 2024, doi.org/10.3390/life14020221, available via: https://www.mdpi.com/2075-1729/14/2/221, CC BY 4.0.
Bypass Surgery
The healthcare provider uses a small piece of tissue from a donor or from another part of the body to build a new route to the compressed portion of the iliac vein. This process restores the typical flow of blood. This is rarely performed and reserved for cases where endovascular treatment fails.
Surgical Resection
Resection of the involved venous segment is extremely rare and not routinely performed in modern practice. It is reserved for patients who fail the endovascular procedures. The healthcare provider performs a procedure to reduce the compression on the left iliac vein by moving the right iliac artery. The physicians then place a piece of tissue between the vein and the artery to decrease the pressure.
If you have DVT due to MTS, the doctors may recommend the following:
- Catheter-directed thrombolysis to dissolve clots
- Blood-thinning medications (anticoagulants) are used to prevent or break down blood clots.
- A vena cava filter, which is a device placed in your inferior vena cava that traps blood clots, so they do not move to your lungs.
Differential Diagnosis
Vein compression can occur due to underlying malignancy, hematoma, cellulitis, or lymphadenopathy. The anatomical variants or disease processes that may compress the iliac vein include:
- Osteophytes (Smooth bony projections that form along joint margins)
- Retroperitoneal fibrosis (an inflammatory disorder characterized by fibrous tissue growth in the abdominal cavity’s back, often surrounding the aorta, iliac arteries, and ureters.
- Aortoiliac aneurysm (dangerous weakening and ballooning of the lower aorta that extends into the iliac arteries).
- Uterine leiomyoma (uterine fibroids).
MTS Prognosis
With timely diagnosis of symptomatic patients and prevention of mechanical compression, most patients with MTS can maintain a high quality of life. It is important to continue intermittent surveillance to address symptom progression. Close follow-up can mitigate thrombotic recurrence and optimize quality of life.
MTS generally does not reduce life expectancy. Most people with this condition have a normal life span and a good quality of life. However, the condition can increase the risk of DVT and PE. These are also manageable with appropriate treatment regimens, such as blood thinners and stenting.
How to Sleep with May Thurner Syndrome?
To sleep comfortably with MTS, you need to follow these guidelines:
- Elevate your legs above the heart level. You can use pillows or a wedge for this; elevation can reduce swelling and improve circulation.
- Sleep on your back or your right unaffected side. It can minimize the pressure on the left iliac vein.
- Establish a consistent light stretching routine before bed.
Conclusion
MTS is the compression of the LCIV by the RCIV. It is a relatively rare vascular disorder seen primarily in young women. Non-invasive imaging, including duplex ultrasound, CT, and MRI, is used to confirm the diagnosis of MTS in patients with symptoms. These imaging techniques play an important role in planning treatment. Minimally invasive treatment regimens, such as angioplasty, stenting, and clot-busting medications, provide safe and effective methods to relieve acute symptoms. These treatment methods also prevent the management of the chronic symptoms associated with PTS. Clinical follow-ups are necessary to prevent the relapse of MTS and its associated complications.
References
[1] Liddell, R. P., & Evans, N. S. (2018). May-Thurner syndrome.Vascular Medicine,23(5), 493-496.
[2] Kaltenmeier, C. T., Erben, Y., Indes, J., Lee, A., Dardik, A., Sarac, T., & Chaar, C. I. O. (2018). Systematic review of May-Thurner syndrome with emphasis on gender differences.Journal of Vascular Surgery: Venous and Lymphatic Disorders,6(3), 399-407.
[3] Mangla, A., & Hamad, H. (2024). May-Thurner Syndrome. InStatPearls [Internet]. StatPearls Publishing.
[4] Wu, W. L. M., Tzeng, W. S., Wu, R. H., Tsai, W. L., Chen, M. C., Lin, P. C., & Tsai, I. C. (2012). Comprehensive MDCT evaluation of patients with suspected May-Thurner syndrome.American journal of roentgenology,199(5), W638-W645.
[5] McDermott S, Oliveira G, Ergül E, Brazeau N, Wicky S, Oklu R. May-Thurner syndrome: can it be diagnosed by a single MR venography study? Diagn Interv Radiol. 2013 Jan-Feb;19(1):44-8.
[6] Radaideh, Q., Patel, N. M., & Shammas, N. W. (2019). Iliac vein compression: epidemiology, diagnosis and treatment.Vascular health and risk management, 115-122.
[7] Mousa, A. Y., & AbuRahma, A. F. (2013). May–Thurner syndrome: update and review.Annals of Vascular Surgery,27(7), 984-995.
[8] Choy, K. T., & Bhutia, S. (2019). Recurrent unilateral cellulitis: is it May-Thurner syndrome (MTS)?.BMJ Case Reports CP,12(7), e229511.
[9] Ono, R., Takahashi, H., Hori, Y., & Fukushima, K. (2021). May-Thurner syndrome with calcified uterine leiomyoma.Internal Medicine,60(14), 2343-2344.