
{kind=link}

thyroidectomy procedure A thyroidectomy is a surgical procedure done to remove the thyroid gland. The important gland can be removed partially or completely, depending on the pathology causing the thyroid issues. Common problems for which surgeons prefer gland excision include goiters and cancers. It is a safe and effective procedure. The surgery has a high success rate for specific thyroid cancers such as papillary thyroid carcinoma, with a 5-year survival rate of more than 95%.
What Is Thyroidectomy?: thyroidectomy procedure
It is a major surgery performed to fix an affected thyroid gland that can not be cured with conservative therapies. The thyroid gland is a butterfly-shaped organ present in your neck. It produces the hormones thyroxine (T4) and tri-iodothyronine, which regulate your body’s metabolism and control growth/development. Thus, dysregulation of gland function leads to metabolic and growth abnormalities in the body.

Thyroid Gland in the Neck
What Are The Indications For A Thyroidectomy?
Healthcare providers opt for a thyroidectomy surgery in different conditions, including:
Goiter
The condition of an enlarged thyroid gland is called goiter. Several pathologies directly impact the thyroid gland and can lead to its enlargement. Very large goiters that cause compression of nearby structures and associated serious complications like dysphagia (swallowing difficulty) and dysphonia (muffled voice) require surgical removal. Clinicians have noted the following diseases to be associated with goiter:
Hashimoto’s Disease:
It is an autoimmune disorder in which your immune cells mistakenly attack the thyroid gland, leading to its destruction. The immune-mediated attack causes inflammation (thyroiditis) and destruction of the gland, which eventually results in underactivity of the thyroid, i.e., hypothyroidism. In the majority of cases, doctors prescribe oral pills containing the deficient hormones (due to hypothyroidism). However, studies show that total thyroidectomy yields improved health-related quality of life and fatigue as compared to medical therapy, but it is not a standard treatment for Hashimoto’s thyroiditis and is only considered in rare cases, such as large compressive goiter or suspicion of malignancy.
Sometimes, even despite adequate substitution of the missing hormones, the patients are plagued with problems like fatigue and body aches. Thus, to attain a symptom-free life, doctors advise a total thyroidectomy. The latest studies have shown that thyroidectomy has an evident symptom-reducing effect on patients with Hashimoto’s thyroiditis and persistent symptoms.
Grave’s Disease:
Another autoimmune disease that affects the thyroid gland is Graves’ disease. Unlike Hashimoto’s thyroiditis, we see hyperactivity of the thyroid gland in this disorder. Hyperthyroidism also leads to goiter that needs medical attention. When compared with antithyroid drugs, thyroidectomy proves to be the better treatment option with higher cure rates and lower risk of recurrence.
According to reports on patient-reported outcomes, thyroid removal surgery significantly improves quality of life and thyroid-specific symptoms in Graves’ patients.
Thyroid Nodules
A thyroid nodule is a common finding in the thyroid gland. These nodules form with the thyroid gland. They are filled with fluid, and enlarged nodules feel like a lump in the neck. Mostly, these growths are benign, but a small percentage can turn malignant. Some nodules cause overproduction of the thyroid hormone. The vast majority of fluid-filled nodules are asymptomatic. However, large thyroid nodules can cause symptoms like hoarseness, difficulty in swallowing, and breathing. Therefore, doctors perform surgery to alleviate symptoms and minimize the chances of conversion into cancer. According to studies, both hemithyroidectomy and total thyroidectomy are effective approaches in the treatment of nodules with a very low rate of post-surgical complications.
Uncontrolled Hyperthyroidism
Overactivity of the thyroid gland releases large quantities of the thyroid hormone into the bloodstream, which leads to issues like rapid heartbeat, unexplained weight loss, and increased sweating, etc. Reports suggest that thyroidectomy can be the right treatment for some patients.
A recent, large clinical study has concluded that the postoperative outcomes of thyroidectomy in patients with uncontrolled hyperthyroidism are good and the procedure is safe.
Thyroid Cancer
A thyroidectomy procedure is frequently adopted to save a patient from the havoc of cancer. Endoscopic surgeries are gaining wide popularity nowadays. Thus, many surgeons prefer an endoscopic approach in dealing with a carcinomatous goiter. Endoscopic thyroid surgery has proven to be an effective and safe choice in thyroid cancer patients. Moreover, hemithyroidectomy evidently improves health-related quality of life in such patients.
Medullary thyroid carcinoma is a rare type of thyroid cancer that is treated with surgical removal of the gland. Researchers have noted that thyroid lobectomy (removal of just a lobe of the gland) yields results similar to total thyroidectomy in some cases. Therefore, doctors must properly analyze the patient’s condition and devise a treatment plan accordingly.
What Are The Different Types Of Thyroidectomy?
Based on the extent of gland removal, thyroidectomy is divided into the following types:
Partial Thyroidectomy
In this surgery, the surgeon removes a specific part of your thyroid gland. It is further divided into different types.
In a hemithyroidectomy, the surgeon removes one of the two lobes of the thyroid gland. As a lobe is removed in this procedure, doctors also call it a thyroid lobectomy. A lobectomy may be indicated in cases of thyroid nodules or cancer affecting only one side (lobe) of the gland.
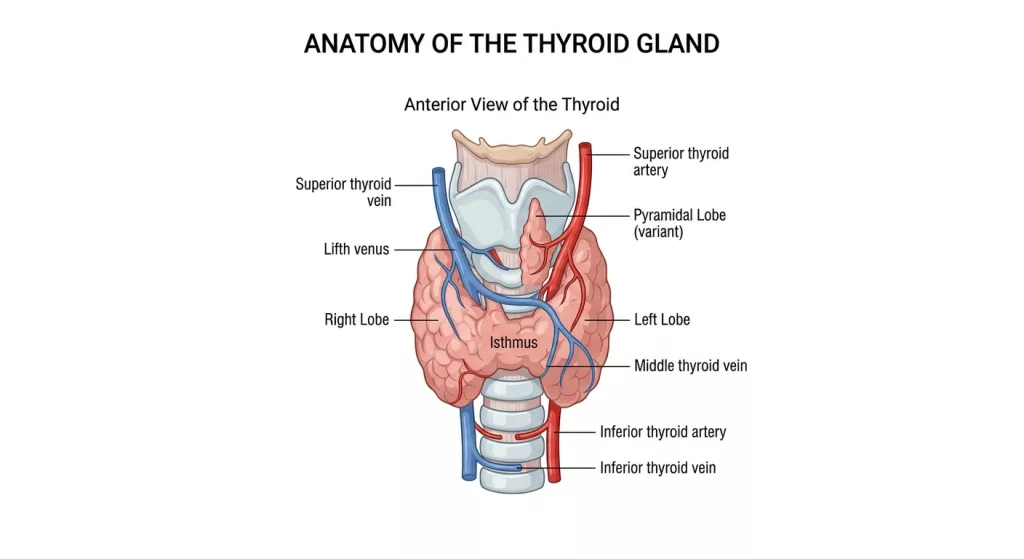
Anatomy of the thyroid gland
In rare cases, doctors remove the bridge connecting the 2 lobes, i.e., the isthmus. Isthmusectomy with bilateral neck dissection can be a feasible approach for selected patients with papillary thyroid carcinoma.
Total Thyroidectomy
As the name indicates, the whole thyroid gland is removed surgically. It offers better symptomatic relief and minimal chances of recurrence. Your healthcare provider will determine which type of surgery suits your condition. It is used in appropriate cases with malignancy, large goiter, or bilateral disease. Recurrence risk depends on the underlying pathology.
Conventional Vs Endoscopic
Thyroidectomy procedures can also be differentiated on the basis of surgical approach. Conventional (open) thyroidectomy involves making an incision in the skin and accessing the gland with conventional instruments. However, now doctors can use fine endoscopic instruments to gain access to the gland via very small cuts in the skin. Endoscopic thyroidectomy has been shown to have similar results to the conventional methods.
The greatest disadvantage of an open thyroidectomy is scar formation. To avoid this. Surgeons now use a transoral approach (through the mouth). Studies show that transoral endoscopic thyroidectomy vestibular approach causes lesser postoperative pain, has a safety profile similar to open thyroidectomy, and is cosmetically superior.
How To Prepare For The Surgery?
As the thyroid gland produces hormones (an endocrine gland), a thyroidectomy is done on the advice of an endocrinologist. Thus, patients are given instructions by an endocrinologist and a surgeon. Your doctor will communicate to you the fact that you will need to take thyroid hormone pills for life after the surgery. The procedure of gland removal is performed after several pre-emptive steps, including:
Diagnostic Tests
Based on your symptoms, doctors perform diagnostic tests to understand the underlying cause of thyroid function dysregulation. A thyroid ultrasound is a reliable imaging test that helps to identify the exact part of the thyroid carrying the abnormal growth (nodule or tumor).
Moreover, your healthcare provider may also perform a pre-hand Fine needle aspiration (FNA) biopsy, i.e., extract some cells from the gland to check for the type of growth (cancerous or benign).
An important test before thyroid surgery is the vocal cord function test. Damage to the laryngeal nerve (the nerve that innervates the vocal cords) is a common complication of this procedure. Therefore, preoperative laryngoscopy is recommended in selected patients, especially those with cancer or prior neck surgery.
Medications
You will need to take your thyroid hormone management drugs before surgery. Doctors prefer achieving a euthyroid state (normal thyroid function) before undergoing thyroidectomy. This is achieved using appropriate medications and helps avoid life-threatening complications like thyroid storm.
A thyroid storm or thyrotoxic crisis is a rare, life-threatening condition in which there is rapid release of excessive thyroid hormone into the blood. Patients experience high fever, agitation, congestive heart failure, and a loss of consciousness.
This phenomenon is mostly observed in patients having hyperthyroidism due to Graves’ disease. However, thyrotoxicosis is also reported in patients undergoing surgery for metastatic papillary thyroid cancer.
Your doctor may also advise you to quit smoking for better healing. You will need to stop blood thinner medicines about a week before the surgery (or as guided by the surgeon).
NPO
You should follow the “nothing by mouth” protocol and not eat/drink (except water) for several hours before the procedure. Your healthcare provider will guide you about fasting.
The Procedure
A thyroidectomy is performed in the following steps:
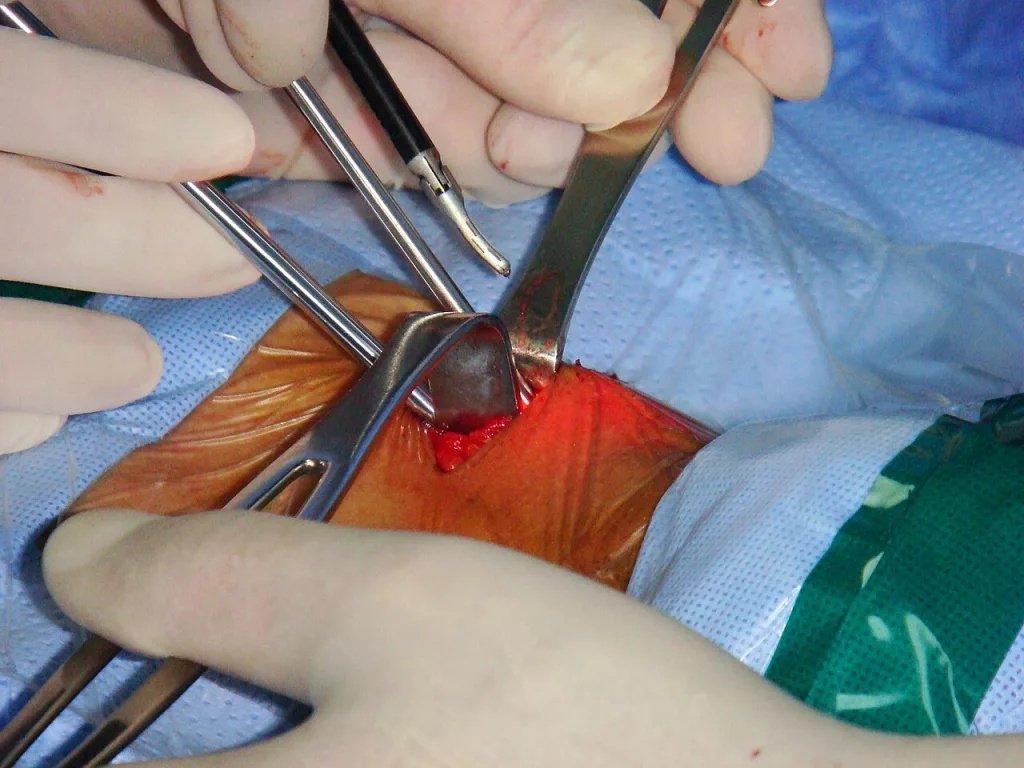
Surgeons performing a minimally invasive video-assisted (MIVAT) thyroidectomy. The endoscopic instrument carries a camera that assists in performing the surgery. Image courtesy ofHaitham Alfalah, available in the public domain, via Wikimedia Commons
- An anesthesiologist will give you general anesthesia via an IV injection. A breathing tube is passed to keep your breathing under control and protect your airway.
- After the anesthesia takes effect, the surgeon marks the surgical site and makes an incision. For open (conventional) surgery, it is a standard incision made on the neck. However, for endoscopic surgery or minimally invasive video-assisted thyroidectomy (MIVAT), it’s a smaller incision made through your mouth, breast, ear, or shoulder blade.
- In rare cases, the surgeon can opt for the sternum as a site for entry.
- After gaining access, surgeons identify the laryngeal nerve and consciously preserve it. Some experts use intraoperative nerve monitoring to minimize the risk of nerve damage.
- Then they cut the faulty gland (partial) or completely remove the thyroid gland.
- The surgeon may also remove some lymph nodes around your gland to collect a sample.
- In the next step, the surgeon closes the incision with stitches (mostly dissolvable).
Lymph node samples are sent to the lab, where pathologists check for any signs of malignancy.
How Long Does It Take For The Procedure To Complete?
A thyroidectomy usually takes 1-3 hours to complete. However, you can see a shorter surgery when doing a partial thyroidectomy. Recovery generally takes 1–2 weeks for routine activities, while full recovery and hormone stabilization may take several weeks to months.
What Happens After A Thyroidectomy?
After recovering from the anesthesia, you can have something light to eat and drink. Patients need to spend the night at the hospital (under the monitoring of a healthcare provider). You may experience a sore throat due to the breathing tube.
After the surgery, you will need to take daily thyroid hormones, i.e., levothyroxine pills, as you have lost the gland that produces the hormone naturally. Patients undergoing total thyroidectomy will also need to take calcium supplements for some time (several weeks) to prevent low blood calcium levels.
In the case of open thyroidectomy, you can expect to see a scar on the surgery site, which heals in 12-18 months after the surgery.
Complications Of Thyroidectomy
Generally, a thyroidectomy surgery is very safe. However, there are some complications associated with it as it is a major surgery. Common complications that may develop after the surgery include:
- Laryngeal nerve injury: This nerve innervates the vocal cords. Damage/injury to the nerve can lead to vocal cord paralysis, dysphonia (raspy, strained voice), and voice hoarseness.
- Low calcium levels: Unintentional damage to the parathyroid glands can lead to hypocalcemia. The condition can develop transiently or permanently.
- Bleeding: Very rarely, excessive bleeding can block your airway and make it hard to breathe.
Final Word
Thyroidectomy is a procedure to remove the thyroid gland. Doctors remove part of (hemithyroidectomy) or complete (total thyroidectomy) of your gland to treat diseases like untreatable goiter, uncontrolled hyperthyroidism, autoimmune thyroiditis (Graves’ disease, Hashimoto’s thyroiditis), nodules, and thyroid cancer. Your surgeon can opt for a conventional approach in which an incision is made in your neck. Modern surgeons perform minimally invasive endoscopic surgeries (assisted via video) in which they approach the gland through the mouth, breast, or ear. The procedure takes one to three hours to complete, and recovery takes two to three weeks. The surgery is effective in alleviating symptoms of nodules, hyperthyroidism, and cancer.
References
[1] Alyousef, M. Y., Ghandour, M. K., Al-Mohawes, M., Alnwaisir, M., Islam, T., & Al Qahtani, K. (2022). Long-term quality of life (5-15 years post-thyroidectomy) of thyroid carcinoma patients in two tertiary care hospitals.Cureus,14(2).
[2] Guldvog, I., Reitsma, L. C., Johnsen, L., Lauzike, A., Gibbs, C., Carlsen, E., … & Søiland, H. (2019). Thyroidectomy versus medical management for euthyroid patients with Hashimoto disease and persisting symptoms: a randomized trial.Annals of internal medicine,170(7), 453-464.
[3] Hoff, G., Bernklev, T., Johnsen, L., Reitsma, L., Sina, D., Lauzike, A., … & Søiland, H. (2024). Thyroidectomy for euthyroid patients with Hashimoto disease and persistent symptoms: an observational, postrandomization study.Journal of Thyroid Research,2024(1), 5518720.
[4] Zheng, X., Zhu, Y., Chen, M. G., Su, Y. C., & Wu, X. M. (2025). Thyroidectomy versus antithyroid drugs in Graves’ disease: a meta-analysis of randomized controlled trials.BMC surgery,25(1), 328.
[5] Gunn, A. H., Frisco, N., Thomas, S. M., Stang, M. T., Scheri, R. P., & Kazaure, H. S. (2022). Patient-reported outcomes following total thyroidectomy for Graves’ disease.Thyroid,32(1), 54-64.
[6] Albano, D., Treglia, G., Dondi, F., Giubbini, R., Galani, A., Cappelli, C., … & Casella, C. (2022). Comparison between total thyroidectomy and hemithyroidectomy in TIR3B thyroid nodules management.Endocrine,78(2), 315-320.
[7] Ergenç, M., Altunsu, S., Zorlu, F. N., Akmercan, A., & Uğurlu, M. Ü. (2025). Thyroidectomy for hyperthyroidism before the euthyroid state: is it safe?.BMC surgery,25(1), 440.
[8] Fazendin, J., Zmijewski, P., Allahwasaya, A., McLeod, C., Akhund, R., Gillis, A., … & Lindeman, B. (2023). Surgical treatment of hyperthyroidism can be performed safely before a euthyroid state is achieved.Thyroid,33(6), 691-696.
[9] Li, X., Ding, W., & Zhang, H. (2023). Surgical outcomes of endoscopic thyroidectomy approaches for thyroid cancer: a systematic review and network meta-analysis.Frontiers in Endocrinology,14, 1256209.
[10] Bach, K., Ansari, P., Ansari, H., Mott, N. M., Elfenbein, D. M., Underwood, H., & Pitt, S. C. (2024). Health-related quality of life in patients with low-risk differentiated thyroid cancer: a systematic review examining the extent of thyroidectomy.Thyroid,34(1), 14-25.
[11] Lincango, E. P., Vilatuna-Andrango, L., Arce-Camposano, A., Mena-García, C., Figueroa, L., Herold, S., … & Brito, J. P. (2026). Total thyroidectomy vs lobectomy for sporadic medullary thyroid cancer: A systematic review and meta-analysis.JAMA Otolaryngology–Head & Neck Surgery,152(4), 400-408.
[12] Dan, J., Tan, J., Guo, Y., Xu, Y., Chen, J., & Huang, J. (2024). Isthmusectomy for papillary thyroid carcinoma in the isthmus: the less the better.Asian Journal of Surgery,47(1), 367-372.
[13] Gupta, K., & Kataria, K. (2024). Comparison of different approaches of endoscopic thyroidectomy and open thyroidectomy: a meta-analysis.Indian Journal of Surgery,86(Suppl 1), 206-219.
[14] Oh, M. Y., Chai, Y. J., Yu, H. W., Kim, S. J., Choi, J. Y., & Lee, K. E. (2023). Transoral endoscopic thyroidectomy vestibular approach as a safe and feasible alternative to open thyroidectomy: a systematic review and meta-analysis.International Journal of Surgery,109(8), 2467-2477.
[15] Kwon, S. H., Kim, M. J., Jung, S. Y., & Jeon, J. H. (2023). Thyroid storm caused by metastatic papillary thyroid carcinoma tissue after total thyroidectomy: a case report.Journal of Yeungnam Medical Science,40(Suppl), S93-S97.