
{kind=link}

Osteoarthritis Rheumatoid Arthritis The term ‘arthritis’ is commonly used synonymously with osteoarthritis. But arthritis is not a single disease; rather, it is an umbrella term used to describe a group of conditions that affect the joints. Among these, osteoarthritis and rheumatoid arthritis are the most common, and most people often confuse these.
The confusion is understandable as both cause joint pain and stiffness in patients, both can involve the hands, and both get worse over time. The underlying biology is completely different, though; one is due to mechanical wear, and the other is because of an autoimmune attack. The diagnosis cannot be mixed up, because treating one with the other’s treatment approach doesn’t work.
What is Arthritis?: Osteoarthritis Rheumatoid Arthritis
The term arthritis means inflammation of a joint; derived from the Greek words ‘arthron’, meaning joint, and ‘itis’, meaning inflammation. We use it loosely to describe any condition that causes joint pain, swelling, or stiffness, even when inflammation is minimal or not the primary driver, as in osteoarthritis.
We can classify arthritis into major categories: degenerative, autoimmune, crystal-induced, infectious, or reactive.
A common misconception is that only the elderly are affected by arthritis; the truth is that it can affect people of all ages, though the prevalence increases with age.
What is Osteoarthritis?
Osteoarthritis is the most common form of arthritis worldwide; it is a degenerative joint disease, commonly seen in the elderly. Some joints are affected more often than others, like the knees, hips, hands (DIP and PIP joints), spine, and base of the thumb.
Risk factors include old age, obesity, previous joint injury, repetitive joint use, female sex, and family history.
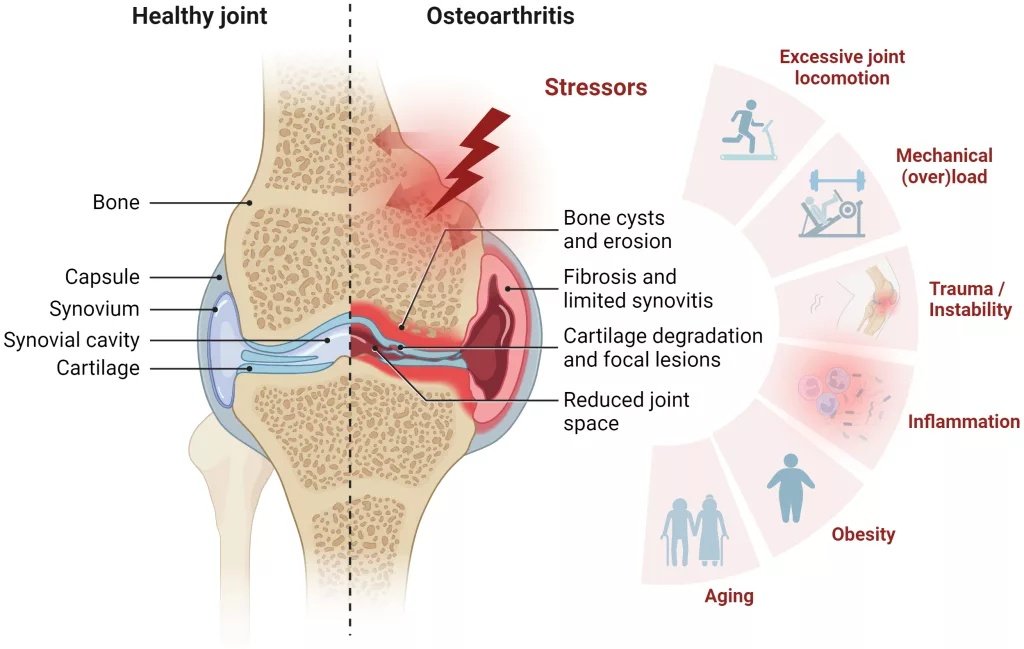
Synovial joint architecture and stressors contributing to osteoarthritis (OA): While healthy joints rely on smooth cartilage and synovial fluid for movement, the pathology in osteoarthritis is defined by cartilage loss, bone spurs, and inflammatory changes driven by factors like mechanical stress and age. (Image Courtesy: Damerau A, Rosenow E, Alkhoury D, Buttgereit F, and Gaber T (2024) Fibrotic pathways and fibroblast-like synoviocyte phenotypes in osteoarthritis. Front. Immunol. 15:1385006. Available fromFrontiersand licensed under CC by 4.0)
How It Develops
The mechanism behind osteoarthritis developing is degenerative, i.e., articular cartilage that cushions the ends of bones in a joint gradually breaks down. This exposes the bone ends, in advanced stages there is increased bone-on-bone contact; this causes pain, stiffness, and loss of movement.
The body tries to repair this by forming new bone at the joint margins: osteophytes[1], or bone spurs, but these instead contribute to deformity and pain. Along with this, the bone under the cartilage (subchondral) also starts changing: it thickens and becomes harder (sclerosis). In some cases, fluid-filled cysts might also form.[2]
What is Rheumatoid Arthritis?
Rheumatoid arthritis is a chronic autoimmune disease, where your own immune system mistakenly attacks your joints, more specifically, the synovial membrane that lines the joints. The joints most frequently involved are the small joints of the hands (MCPs and PIPs), wrists, ankles, and feet.[3] The involvement is classically symmetrical; that is, when a joint is involved, it does so on both sides of the body. The one joint notably spared in most cases is the DIP (distal interphalangeal joint), which is a clear differentiator from OA.
Risk factors include female sex (3:1), it most commonly presents between 40–60 years of age, smoking, family history, and HLA-DR4 genetic association.[4]
How It Develops?
When the immune system attacks the synovium, it results in inflammation (synovitis). If not treated, this inflammation persists over time and damages the cartilage and bone. The inflamed synovium thickens to form a pannus that erodes the cartilage and bone from the inside.
Unlike osteoarthritis, though, it affects the whole body, not just the joints. Extra-articular features include rheumatoid nodules, lung involvement, cardiovascular disease, and anaemia.
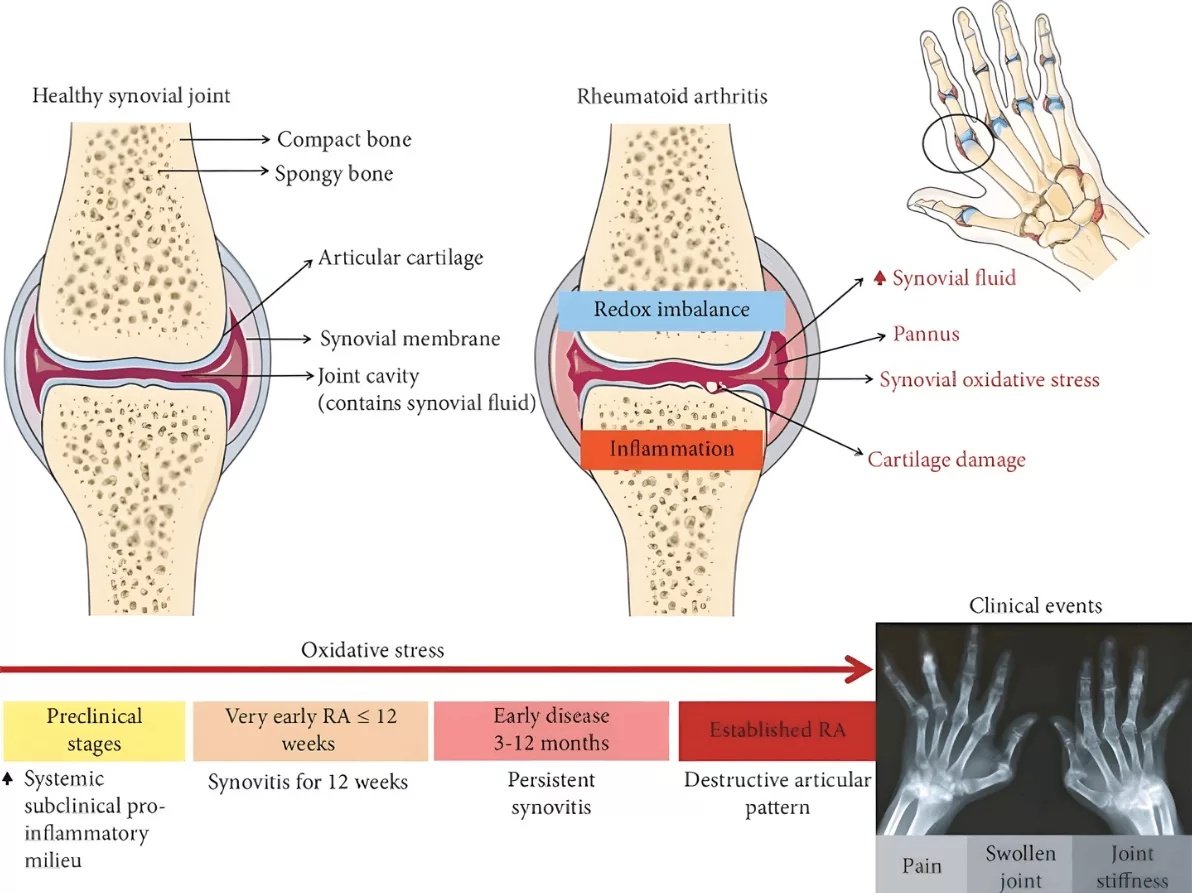
The timeline of rheumatoid arthritis (RA)begins with a subclinical proinflammatory phase in which there are circulating autoantibodies, years before clinical symptoms appear. As inflammation and oxidative stress intensify, patients experience joint pain, swelling, and prolonged morning stiffness. Without early intervention, this inflammatory process leads to irreversible articular damage, joint destruction, and functional disability. (Image Courtesy: Fonseca, Lucas José Sá da, Nunes-Souza, Valéria, Goulart, Marília Oliveira Fonseca, Rabelo, Luiza Antas, Oxidative Stress in Rheumatoid Arthritis: What the Future Might Hold regarding Novel Biomarkers and Add-On Therapies, Oxidative Medicine and Cellular Longevity, 2019, 7536805, 16 pages, 2019. Available fromWileyand licensed under CC by 4.0)
How Osteoarthritis and Rheumatoid Arthritis Differ:
Overall, the two conditions only share one thing in common: arthritis. Everything else presents a clear difference.
| Osteoarthritis | Rheumatoid Arthritis | |
|---|---|---|
| Mechanism | Cartilage breakdown from mechanical and biological factors | Immune mediated synovial inflammation |
| Onset | Gradually, over years | Can be subacute, developing within weeks sometimes, with a sudden flare |
| Age of Onset | Over 50 years of age | Peaks at 40-60, but affects all ages including children (juvenile idiopathic arthritis)5Tuomi, A. K., Rebane, K., Arnstad, E., Berntson, L., Fasth, A., Glerup, M., Herlin, T., Kautiainen, H., Nordal, E. B., Peltoniemi, S., Rygg, M., Rypdal, V., Zak, M., & Aalto, K. (2025). Age at diagnosis as a prognostic factor in selected categories of juvenile idiopathic arthritis. RMD open, 11(2), e005369. |
| Symmetry | Not necessarily symmetrical | Characteristically symmetrical: affects joints of both sides |
| Morning stiffness | Lasts less than 30 minutes and eases with movement | Lasts more than an hour, might even be several hours |
| Systemic symptoms | No systemic manifestations related to OA itself | RA causes fatigue, fever, weight loss, malaise |
| Joint swelling | OA joints may be bony and hard than warm and soft | More pronounced due to active inflammation |
| DIP vs MCP involvement | Distal and proximal interphalangeal joints (DIPs and PIPs) are more commonly involved | Affects metacarpophalangeal and proximal interphalangeal joints (MCPs and PIPs), and also wrists, classically spares DIPs |

Clinical presentation of hand osteoarthritis, showing Heberden’s nodes at the distal interphalangeal (DIP) joints and Bouchard’s nodes at the proximal interphalangeal (PIP) joints, both of which are hallmark bony swellings associated with the degenerative changes in osteoarthritis. (Image Courtesy: Medvec A R, Shrestha S, Schroeder L L (June 27, 2021) Unusual Stroke-Like Symptoms in a Patient With Generalized Osteoarthritis. Cureus 13(6): e15951. Available fromCureusand licensed under CC by 4.0)
Clinical signs
Even if the rest of the symptoms and presentation is indistinguishable, the clinical signs in joints of the hand are where the distinction is most visible.
In osteoarthritis, we see:
- Heberden’s nodes, which are bony swellings at DIP joints caused by osteophyte formation
- Bouchard’s nodes, same swellings as Heberden’s, but at the PIP joints
- OA of the first carpometacarpal joint gives the base of the thumb a specific squared-off appearance
- On palpation, the joints feel hard and bony, not warm or soft
- Reduced grip strength and pinch grip in advanced cases
In rheumatoid arthritis on the other hand, DIPs are spared, and the signs are quite distinct:
- Ulnar deviation at the MCPs is one the most recognizable deformities, and it results because of joint destruction and tendon imbalance, making the fingers drift towards the little finger side (ulnar)
- Another classic sign is the swan-neck deformity: hyperextension at the PIP with flexion at the DIP, caused by imbalance between flexor and extensor tendons
- Boutonnière deformity is essentially the opposite of swan-neck: flexion at PIP with hyperextension at DIP
- Z-thumb deformity: hyperextension at the IP joint with flexion at the MCP of the thumb
- Visible swelling over the outer (dorsal) wrist because of synovitis
- Firm subcutaneous nodules over pressure points, like the elbow, called rheumatoid nodules
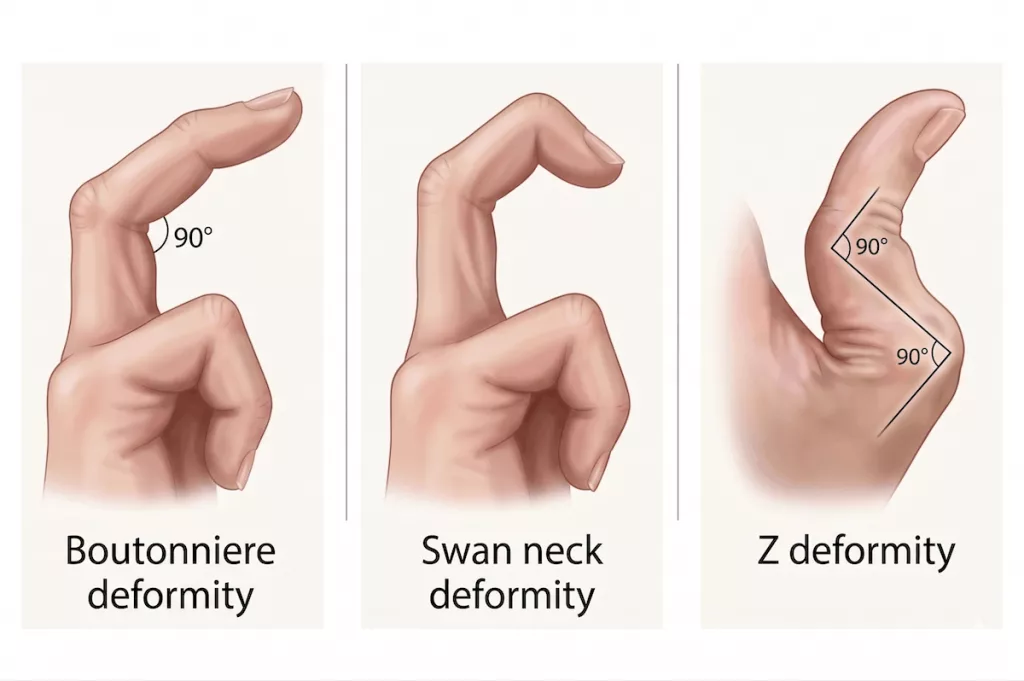
Three specific joint deformities of the hand that are often associated with rheumatoid arthritis. From left to right:Boutonniere deformity(hyperextension of the distal joint and flexion of the middle joint),Swan neck deformity(flexion of the distal joint and hyperextension of the middle joint), andZ deformity(severe zig-zag alignment of the thumb joints)
Radiology Findings:
X-rays are the imaging of choice for arthritis and the findings are mostly distinct enough. The single most important distinguishing point is bone formation (osteophytes) vs bone destruction (erosions). These two findings are mutually exclusive. Also, distribution varies: OA changes are seen at DIPs, RA changes at MCPs and wrists.
In cases of osteoarthritis, we have a classic quartet:
- There is visible joint space narrowing: loss of cartilage space between bones, asymmetric
- Subchondral sclerosis is visible as increased density (white) of the bone just beneath the cartilage
- Osteophytes appear as irregular bony projections
- Subchondral cysts appear as lucent (dark) fluid-filled areas in the bone
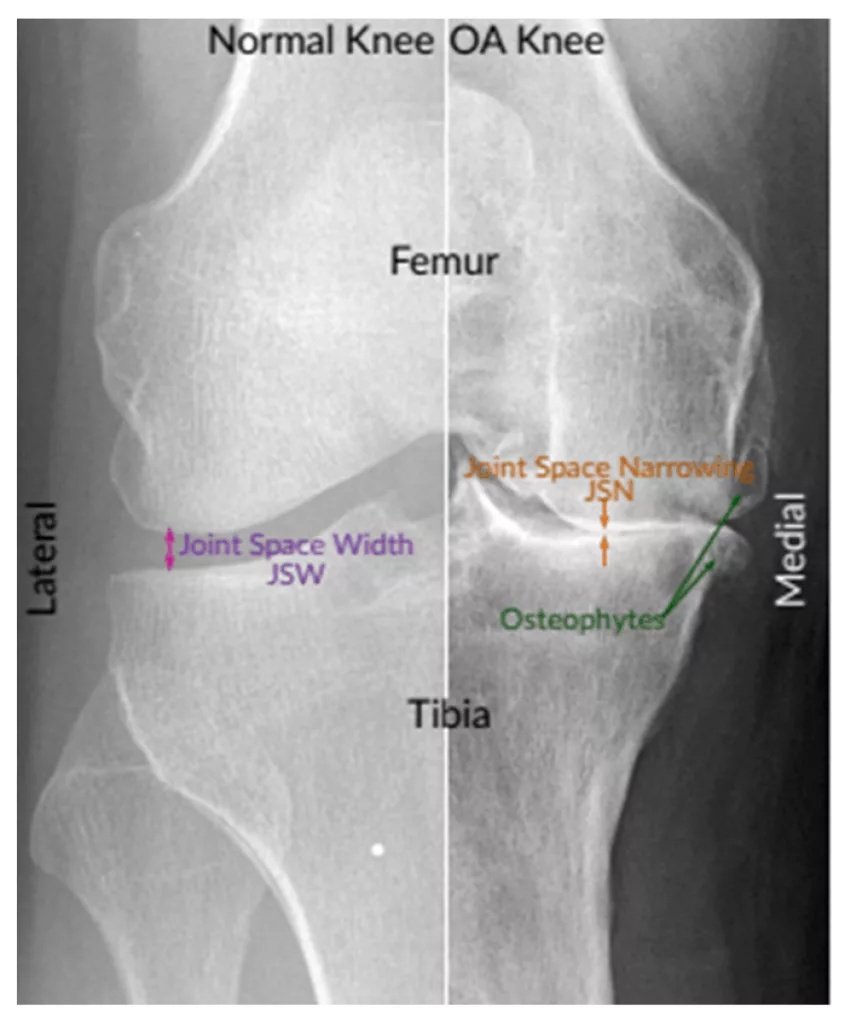
Radiographic comparison of a healthy knee versus a knee with severe osteoarthritis (OA)The normal joint (left) displays normal joint compartments and a clear joint space, while the OA-affected joint (right) shows classic radiographic findings of degeneration: significant joint space narrowing (JSN) and the presence of prominent osteophytes (bone spurs) (Image Courtesy: Ahmed, S. M., & Mstafa, R. J. (2022). Identifying Severity Grading of Knee Osteoarthritis from X-ray Images Using an Efficient Mixture of Deep Learning and Machine Learning Models. Diagnostics, 12(12), 2939. Available fromMDPIand licensed under CC by 4.0)
Joints affected by rheumatoid arthritis, on the other hand, have a distinct appearance on radiography:
- Periarticular osteopenia is one of the earliest signs. The reduced bone density around the affected joints is visible as less white
- Another early finding is an increased soft tissue shadow around the affected joints because of swelling
- Joint space narrowing is visible in RA as well, but is usually symmetrical (on both sides)
- The hallmark signs, however, are erosions, which appear as small punched-out defects at the joint margins.
- In advanced stages, the swan neck and ulnar deviation deformities are also visible on radiology
Laboratory Findings
There are no specific blood markers for osteoarthritis, and that itself is diagnostically useful. Normal blood tests in a patient with joint pain support OA over an inflammatory cause. Even ESR and CRP are normal or only mildly elevated. If synovial fluid is aspirated and analysed, it is non-inflammatory in case of OA: clear, white cell count < 2000/mm.
This can be useful if the diagnosis is still uncertain, because in RA, synovial fluid shows clear inflammation: turbid, high white cell count. Other findings in RA can be:
- Rheumatoid factor (RF): an antibody that is positive in 70-80% of RA patients.[5] However, despite the name, it is not specific to RA. In fact, it can be positive in other inflammatory conditions, and sometimes even in healthy elderly patients.
- Anti-CCP antibodies are highly specific (~90–95%), and can actually be positive years before symptoms develop
- If either RF or anti-CCP is positive, the disease is termed seropositive and is associated with more aggressive disease. When both are negative (seronegative), it doesn’t necessarily mean a milder form of the disease, but that the diagnosis has to be clinical.
- Unlike osteoarthritis, ESR and CRP are elevated in active RA, reflecting systemic inflammation. More than diagnosis, this is used to monitor disease activity.

Radiographic progression of rheumatoid arthritis (RA) over 13 years: Panel (a) early disease, showing narrowing of the radiocarpal and carpometacarpal joints, along with a bone cyst, and on the other hand, Panel (b) reveals advanced disease progression, with severe erosions, joint destruction, and juxta-articular osteoporosis (Image Courtesy: Żelnio, E., Taljanovic, M., Mańczak, M., & Sudoł-Szopińska, I. (2023). Hand and Wrist Involvement in Seropositive Rheumatoid Arthritis, Seronegative Rheumatoid Arthritis, and Psoriatic Arthritis—The Value of Classic Radiography. Journal of Clinical Medicine, 12(7), 2622. Available fromMDPIand licensed under CC by 4.0)
Diagnosis
Both of these diseases have a largely clinical diagnosis, though imaging and lab tests can be used to support it. Especially for OA, clinical history and X-ray findings are usually enough.
In case of RA, the ACR/EULAR 2010 classification criteria include scoring for joint involvement, serology, inflammatory markers, and duration of symptoms.
| Domain | Category | Score |
|---|---|---|
| Joint Involvement | 1 large joint | 0 |
| 2–10 large joints | 1 | |
| 1–3 small joints | 2 | |
| 4–10 small joints | 3 | |
| >10 joints (at least 1 small) | 5 | |
| Serology | Negative RF and negative ACPA | 0 |
| Low positive RF or low positive ACPA | 2 | |
| High positive RF or high positive ACPA | 3 | |
| Acute-Phase Reactants | Normal CRP and normal ESR | 0 |
| Abnormal CRP or abnormal ESR | 1 | |
| Duration of Symptoms | < 6 weeks | 0 |
| ≥ 6 weeks | 1 |
2010 ACR/EULAR classification criteria for rheumatoid arthritis.This scoring system evaluates joint involvement, serology (RF and ACPA status), acute-phase reactants (CRP and ESR), and symptom duration to aid in clinical diagnosis. A total score of 6 or higher out of 10 indicates definite rheumatoid arthritis, provided that synovitis is present and no alternative diagnosis better explains the findings.7Aletaha, D., Neogi, T., Silman, A. J., Funovits, J., Felson, D. T., Bingham, C. O., 3rd, Birnbaum, N. S., Burmester, G. R., Bykerk, V. P., Cohen, M. D., Combe, B., Costenbader, K. H., Dougados, M., Emery, P., Ferraccioli, G., Hazes, J. M., Hobbs, K., Huizinga, T. W., Kavanaugh, A., Kay, J., … Hawker, G. (2010). 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis and rheumatism, 62(9), 2569–2581.
During the early stages, serology might come out to be negative, and changes might not be visible on X-rays. In this case, MRI and ultrasound can usually detect synovitis and erosions. Ultrasounds are, in fact, becoming routine in rheumatology clinics to detect active synovial inflammation and guide treatment injections.
Treatment and Management
Since the underlying causes, mechanisms and changes are so different, the treatment strategies of both these conditions do not overlap, save for simple pain management.
Osteoarthritis
OA cannot be fully prevented or treated but progression can be slowed and onset delayed. Management is purely symptomatic, no disease-modifying option exists.[6]
- Clinicians recommend lifestyle changes like weight loss, low-impact exercise, and physiotherapy. For knee OA, weight management is actually the most evidence-based intervention. Every kg of body weight adds roughly 4kg force on the knee.[7].
- For pain, the first-line drug is paracetamol or NSAIDs. Duloxetine is recommended later for chronic pain.
- Intra-articular corticosteroid injections are popularly used for short-term relief. Other intra-articular injections include hyaluronic acid, though evidence for that is limited.
- For end-stage disease, the only definite treatment is joint replacement; hip and knee replacement surgeries are among the most successful elective procedures.
Rheumatoid Arthritis
For RA, the modern standard is to aim for remission or low-activity disease. Disease-modifying antirheumatic drugs (DMARDs) are the cornerstone of treatment, used to suppress the immune attack and prevent joint damage. These include methotrexate, hydroxychloroquine, sulfasalazine, etc.
- First-line DMARD in most patients is a weekly dose of methotrexate, but it needs the patient to be supplemented with folic acid and regular blood monitoring.[8]
- Newer biological DMARDs are used when the conventional ones fail. TNF inhibitors (infliximab), IL-6 inhibitors (tocilizumab), or B-cell depletion (rituximab). JAK inhibitors (tofacitinib, baricitinib) are newer synthetic DMARDs.
- Because of side effects, corticosteroids are used sparingly, not as treatment but for flares and as bridging therapy.
Final Words
OA and RA both affect quality of life, but RA affects life expectancy as well, since it has extra-articular effects as severe as cardiovascular involvement. That said, there is a window of opportunity: if treatment for RA is started within the first 3-6 months of symptom onset, there is a better outcome for the patient.[9]
It cannot be overstated that any joint pain lasting more than 6 weeks should be assessed properly. A patient who waits for 12 months to see a doctor because they assumed the joint pain was just aging may have developed irreversible erosions because of RA.
In regards to OA, we can try to slow it with weight management and muscle strengthening, but there is no definite treatment. That said, joint replacement is no longer a last resort; it can genuinely improve quality of life in a patient.
References
[1] Hacking C, Osteophyte. Reference article, Radiopaedia.org
[2] Dudaric, L., Dumic-Cule, I., Divjak, E., Cengic, T., Brkljacic, B., & Ivanac, G. (2023). Bone Remodeling in Osteoarthritis-Biological and Radiological Aspects. Medicina (Kaunas, Lithuania), 59(9), 1613.
[3] Mohammed RH, Bhutta BS. Hand and Wrist Rheumatoid Arthritis. [Updated 2023 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560890/
[4] Fugger, L., & Svejgaard, A. (2000). Association of MHC and rheumatoid arthritis. HLA-DR4 and rheumatoid arthritis: studies in mice and men. Arthritis research, 2(3), 208–211.
[5] Tuomi, A. K., Rebane, K., Arnstad, E., Berntson, L., Fasth, A., Glerup, M., Herlin, T., Kautiainen, H., Nordal, E. B., Peltoniemi, S., Rygg, M., Rypdal, V., Zak, M., & Aalto, K. (2025). Age at diagnosis as a prognostic factor in selected categories of juvenile idiopathic arthritis. RMD open, 11(2), e005369.
[6] Wilson D. (2006). Rheumatoid factors in patients with rheumatoid arthritis. Canadian family physician Medecin de famille canadien, 52(2), 180–181.
[7] Aletaha, D., Neogi, T., Silman, A. J., Funovits, J., Felson, D. T., Bingham, C. O., 3rd, Birnbaum, N. S., Burmester, G. R., Bykerk, V. P., Cohen, M. D., Combe, B., Costenbader, K. H., Dougados, M., Emery, P., Ferraccioli, G., Hazes, J. M., Hobbs, K., Huizinga, T. W., Kavanaugh, A., Kay, J., … Hawker, G. (2010). 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis and rheumatism, 62(9), 2569–2581.
[8] Chaplin, S. (2023). NICE on the diagnosis and management of osteoarthritis. Prescriber, 34(2), 15-16.
[9] Messier, S. P., Gutekunst, D. J., Davis, C., & DeVita, P. (2005). Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis and rheumatism, 52(7), 2026–2032
[10] Friedman, B., & Cronstein, B. (2019). Methotrexate mechanism in treatment of rheumatoid arthritis. Joint bone spine, 86(3), 301–307.
[11] Demoruelle, M. K., & Deane, K. D. (2012). Treatment strategies in early rheumatoid arthritis and prevention of rheumatoid arthritis. Current rheumatology reports, 14(5), 472–480.