
{kind=link}

Osteoma It Symptoms You feel a hard, bony lump on your forehead. It doesn’t hurt or move. You press it, and it is nearly as hard as the skull itself. So what is it? Most likely, it might be an osteoma, which is a benign bone tumor that silently develops on the skull and on other bones without the majority of people being aware of its presence.
It is important to know what an osteoma is, more than you may think. Most people do not know that these growths are very prevalent. Although they rarely result in severe damage, they may occasionally cause serious complications.
What Is Osteoma? : Osteoma It Symptoms
An osteoma is a benign bone tumor that typically forms on the skull. The word “benign” means it is not cancerous. Osteomas are made of bone and may be spongy, dense, or even a combination of both. They are benign; hence, they will not spread to other parts of your body.[1]
These are slow-growing tumours. Very slowly, in fact. Some stay the same size for years. Others grow so gradually that a person only notices them after a decade. Osteoma can occur at any age, but it may most commonly affect people aged 30 to 50 years old. It may also occur more frequently in people assigned male at birth.
There are three basic structural types:
- Compact (ivory): Composed of extremely dense bone with almost no marrow spaces
- Spongy (cancellous): Similar in structure to normal bone, often containing bone marrow
- Mixed: A combination of both compact and spongy bone
Paranasal sinus osteomas are found in 3 to 6.4% of CT scans performed for sinus conditions. That statistic alone tells you these growths are far from rare.
The Different Types of Osteoma You Should Know
Not all osteomas are the same. Where they grow, what they look like, and how they behave vary widely depending on the type.
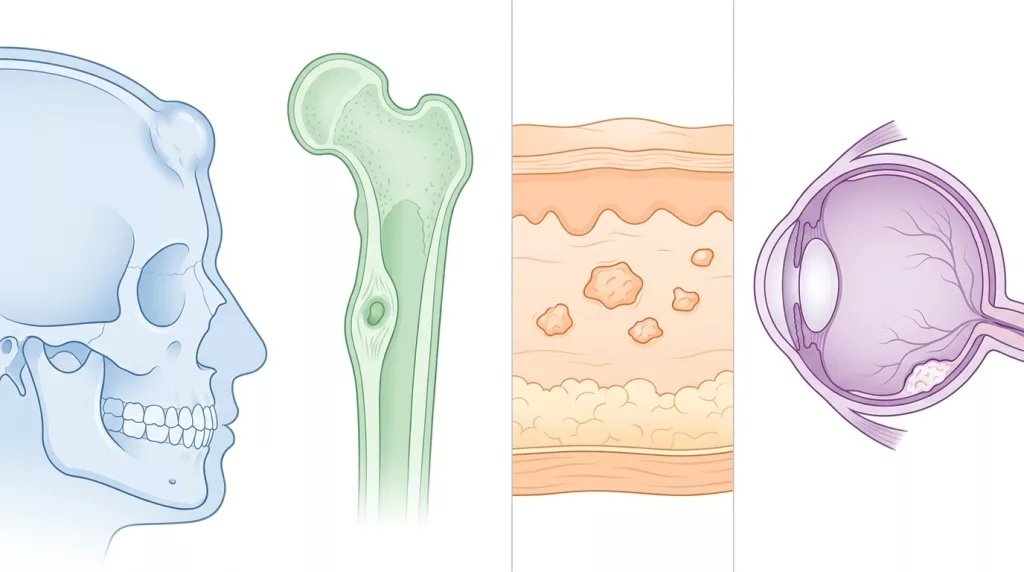
Osteomas can develop in different parts of the body, including the skull and bones
Osteoma of the Forehead and Skull
When it is on your forehead and skull, you may experience headaches. The osteoma of the forehead is one of the most visible types. It often appears as a smooth, hard bump beneath the skin. People sometimes mistake it for a cyst or an old injury.[2]
Larger craniofacial osteomas may cause facial pain, headache, and infection due to obstructed nasofrontal ducts. Craniofacial type often presents with ocular signs and symptoms such as proptosis.
An osteoma skull lesion is typically found on the outer surface of the frontal or parietal bone. Most are discovered by accident during a CT scan or MRI done for another reason. Most skull base osteomas develop for unknown reasons and cannot be conclusively linked to an underlying medical condition or a known risk factor.
Osteoid Osteoma
Osteoid osteoma is a distinct subtype. It doesn’t behave like an osteoma on the skull. Osteoid one is a benign bone-forming tumor that has no potential to become malignant. It classically causes severe pain at night, and that pain is relieved with nonsteroidal anti-inflammatory medications.[3]
Osteoid osteomas tend to be small, measuring less than 1.5 cm in size, and they do not grow. They do, however, typically cause reactive bone to form around them.
The most common symptom of an osteoid type is pain not caused by an injury. The pain is often achy and dull. It often tends to get worse at night. It may even wake you from sleep.
Many young patients have their pain dismissed as growing pains. Unlike growing pains, physical activity has no effect on the pain of osteoid osteomas. This is an important distinction.
Osteoma Cutis
Osteoma cutis is a rare variant. This is an osteoma in which bone tissue develops within the skin. Rather than growing on a bone, the body deposits actual bone tissue inside the skin layers. It can appear as tiny, hard nodules on the face, scalp, or elsewhere. In some cases, it is a primary condition. In others, osteoma cutis may occur as a secondary effect of underlying skin cancer. That’s why any unexplained skin hardening should be assessed by a dermatologist.[4]
Choroidal Osteoma
This type is in a category of its own. Choroidal osteoma grows inside the eye. It is a benign ossifying tumor characterized by mature bone replacing the choroid. The condition affects females more than males and typically first manifests in the teenage years or in the early twenties.[5]
Clinical manifestations include mild blurred vision to severe loss of vision, plus metamorphopsia (distorted vision) and changes to the visual field. It’s a very rare tumor, the cause of which is still unknown.
The most feared complication of choroidal type is not the tumor itself. It is the formation of a choroidal neovascular membrane, which can severely damage the central retina if left untreated.
Common Locations and Their Symptoms at a Glance
The table below summarizes the most frequent locations and the symptoms each may produce.
| Location | Type | Common Symptoms |
|---|---|---|
| Forehead / Skull | Osteoma skull | Hard lump, headaches, cosmetic concern |
| Paranasal sinuses | Skull osteoma | Sinus infections, congestion, blocked drainage |
| Long bones (tibia/femur) | Osteoid osteoma | Night pain, joint stiffness, swelling |
| Skin layers | Osteoma cutis | Hard skin nodules, cosmetic concern |
| Eye (choroid) | Choroidal osteoma | Blurred vision, distorted vision, visual field loss |
| Ear canal | Skull osteoma | Temporaryhearingloss |
| Jawbone | Skull osteoma | Facial pain, difficulty chewing |
| Spine | Osteoid osteoma | Scoliosis, back pain, nerve symptoms |
What Causes Osteoma?
This is where medicine still has gaps. Scientists believe a small percentage of cases may be related to an inherited disorder known as Gardner syndrome, which is an autosomal dominant familial disorder.[6]
The presence of multiple osteomas is suggestive of Gardner syndrome, a variant of familial adenomatous polyposis (FAP) that is characterized by colorectal adenomas, osteomas, and benign skin tumors. It is caused by mutations in the APC gene.
Outside of Gardner syndrome, contributing factors may include:
- Genetic predisposition in some individuals
- Past trauma or injury to bone tissue
- Prior infection at the bone site
- Abnormal bone cell growth during development
Researchers don’t know the exact cause of osteoid osteoma. Causes may include abnormal growth of cells in your body, inflammation in your bone, or injury to the area where the tumor occurs.
Hard Forehead Lumps: When Should You Be Concerned?
Most people who notice hard forehead lumps panic immediately. The good news is that most of these lumps are harmless. You might notice a hard lump on your head before you experience any symptoms. If you have an osteoma tumor, you may not need treatment.
That said, not every hard forehead lump is an osteoma. Other possibilities include epidermoid cysts, lipomas, or, in rare cases, more serious conditions. Any new, unexplained hard lump on the skull or forehead deserves medical evaluation.
Signs that a hard lump on the forehead warrants prompt medical attention:
- It has grown noticeably in a short time
- It causes persistent headaches
- It feels warm or tender to the touch
- You experience changes in vision or hearing
- There is numbness or neurological symptoms nearby
How Is Osteoma Diagnosed?
According to Stanford Medicine, a CT scan of the bones is often enough to diagnose osteoma. In many cases, a biopsy is not necessary.[7]
The diagnostic process typically starts with a physical exam and history. From there, the doctor may order:
- CT scan: The gold standard for osteoma imaging. The characteristic finding on a CT scan for osteoid osteoma is a target-shaped nidus. For skull osteomas, CT shows precise size and location without contrast enhancement.
- X-ray: Useful for osteoid osteomas in long bones. An X-ray of the painful area may reveal thickened bone surrounding a small central core of lower density, which is a distinctive characteristic of the tumor.
- MRI: Less reliable than CT for osteoid osteoma diagnosis. Bone marrow edema appreciated on MRI can mask the typical features of the tumor, and therefore, MRI is less useful than CT for the evaluation of osteoid osteomas.
- Bone scan: Uses a small amount of radioactive tracer to locate osteomas across the head and neck area.
Because osteomas are not cancerous, a biopsy is not needed to confirm the diagnosis.
Osteoma Removal: Treatment Options Explained
When Treatment Is NOT Needed
Most osteomas never require treatment. Osteomas tend to grow slowly; therefore, a wait-and-watch approach may be appropriate for a small, asymptomatic tumor. Doctors call this “watchful waiting.” Regular follow-up imaging ensures the growth isn’t changing rapidly.
When to Consider Osteoma Removal?
Osteoma removal becomes necessary when:
- The tumor causes chronic pain or headaches
- There is sinus obstruction or repeated sinus infections
- It affects vision, hearing, or chewing
- The cosmetic impact is significant to the patient
Surgical Approaches
In some cases, your doctor may be able to remove the tumor by going through the nostrils using the Expanded Endonasal Approach (EEA), a minimally invasive surgical technique that gives you a shorter hospital stay, faster recovery, and no scarring.[8]

Minimally invasive surgery is used to remove a sinus osteoma
For osteomas near the skin surface, doctors can often create small incisions in the skin to remove the growth. Large growths may require more invasive techniques.
Radiofrequency Ablation (RFA)
For osteoid osteoma specifically, CT-guided drill resections and radiofrequency ablations are less invasive choices. An interventional radiologist can do these procedures. Your care team will use a CT scan to precisely locate the osteoid osteoma. The doctor will then use a special drill or heated probe to remove or destroy it.
After radiofrequency ablation, most patients have resolution of their symptoms within 24 hours.
Non-Surgical Pain Management
For those managing osteoid osteoma without surgery, NSAIDs can be nonprescription (aspirin, ibuprofen, or naproxen) or prescription. NSAIDs help to relieve pain and may speed the shrinkage of the osteoid osteoma. With this conservative treatment, symptoms usually end within 33 months.[9]
Treating Choroidal Osteoma: A Different Approach
The management of choroidal osteoma is more complex. The management of choroidal osteoma includes prevention of tumor growth, induction of decalcification of the tumor, and treatment of choroidal neovascularization. There is currently no known systemic metabolic or hormonal method for altering the growth of the choroidal osteoma.[10]
For neovascular membranes, the treatment of choice is anti-angiogenic intravitreal injections, as it is for other causes of choroidal neovascularization. Laser photocoagulation and photodynamic therapy are also used in specific cases.
Prognosis: What to Expect Long-Term
The prognosis of individuals with osteoma is often very good. Osteomas are benign and slow-growing, which implies that they have a good prognosis, and therefore, you can be treated effectively.[11]
No known instances of osteoma turning cancerous have occurred as well. Most patients can lead normal lives without recurrence, once treated. Nevertheless, recurrences are not exceptional, especially following curettage or mere tumor enucleation, hence the choice of complete surgical resection in the event of surgery.
For osteoid osteoma in children and young adults, the prognosis is especially positive. Once treated, people with an osteoid osteoma usually live long, full lives.
When to See a Doctor About Osteoma?
Several individuals carry osteomas for many years without being aware. However, some symptoms warrant an immediate appointment with your doctor or specialist:
- A recent, hard, painless lump on the skull, forehead, or jaw that cannot be explained by a recent trauma.
- Bone pains that continually get better at night and are not relieved by rest.
- Repeated sinus infections, which have no other apparent cause.
- Unexplained changes in vision, especially in young women
- Numbness, auditory alterations, or eye protrusion in or around a known or suspected bone growth.
Early diagnosis implies more choices and fewer possibilities to develop complications.
Summary: Osteoma Can Be Treated and is Mostly Manageable
Knowing what an osteoma is provides patients and their families with the understanding that they can make smart choices. It may be obvious on the forehead, a painful osteoid osteoma in a long bone, osteoma cutis of the skin, a rarer condition, the vision-threatening choroidal osteoma; these are conditions that are well known to medical science.
The majority of osteomas are only to be observed. Others require less invasive and simpler procedures. A few require surgery. The point is not to disregard unexplained hard lumps or chronic bone pain, particularly night pain. When it is necessary, it is safer and more effective to remove the osteoma with early detection and appropriate imaging.
References
[1] Kaplan, I., Nicolaou, Z., Hatuel, D., & Calderon, S. (2008). Solitary central osteoma of the jaws: A diagnostic dilemma.Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 106(3), e22–e29.
[2] Summers, L. E., Mascott, C. R., Tompkins, J. R., & Richardson, D. E. (2001). Frontal sinus osteoma associated with cerebral abscess formation: A case report.Surgical Neurology, 55(4), 235–239.
[3] Rosenthal, D. I., Hornicek, F. J., Torriani, M., Gebhardt, M. C., & Mankin, H. J. (2003). Osteoid osteoma: Percutaneous treatment with radiofrequency energy.Radiology, 229(1), 171–175.
[4] Moritz, D. L., & Elewski, B. (1991). Pigmented postacne osteoma cutis in a patient treated with minocycline: Report and review of the literature.Journal of the American Academy of Dermatology, 24(5), 851–853.
[5] Shields, C. L., Shields, J. A., Augsburger, J. J., & Donoso, L. A. (1988). Choroidal osteoma.Survey of Ophthalmology, 33(1), 17–27. https://doi.org/10.1016/0039-6257(88)90069-0
[6] Gardner, E. J. (1951). A genetic and clinical study of intestinal polyposis, a predisposing factor for carcinoma of the colon and rectum.American Journal of Human Genetics, 3(2), 167–176. PMID: 14902760
[7] Davies, M., Evans, R., Woodhouse, N., & Archbold, H. (2009). Computed tomography in the diagnosis of osteoid osteoma.The Bone & Joint Journal, 91-B(Suppl I), 137.
[8] Lindner, N. J., Ozaki, T., Roedl, R., Gosheger, G., Winkelmann, W., & Wörtler, K. (2001). Percutaneous radiofrequency ablation in osteoid osteoma.Journal of Bone and Joint Surgery (British Volume), 83(3), 391–396.
[9] Raskas, D. S., Graziano, G. P., Herzenberg, J. E., & Heidelberger, K. P. (1992). Osteoid osteoma and osteoblastoma of the spine.Journal of Spinal Disorders, 5(2), 204–211.
[10] Shields, C. L., Materin, M. A., Mehta, S., Foxman, B. T., & Shields, J. A. (2008). Regression of extrafoveal choroidal osteoma following photodynamic therapy.Archives of Ophthalmology, 126(1), 135–137.
[11] Fabbri, N., & Gambarotti, M. (2016). Osteoid osteoma. In C. D. M. Fletcher, J. A. Bridge, P. C. W. Hogendoorn, & F. Mertens (Eds.),WHO Classification of Tumours of Soft Tissue and Bone(4th ed., pp. 270–271). IARC Press.