
{kind=link}

Paragonimiasis Comprehensive Guide Paragonimiasis is a parasitic infection that many people may not be aware of, yet it affects millions worldwide. It is a food-borne disease, which is caused by parasitic flatworms belonging to the genus Paragonimus, commonly known as lung flukes. The infection is a serious health concern in the endemic areas.
Paragonimiasis affects more than 20 million people worldwide, with the highest prevalence in Asia, West Africa, and parts of Central and South America.Paragonimus kellicotti) in the Context of Global Paragonimiasis. Clin Microbiol Rev. 2009;22(3):415-446. doi:10.1128/CMR.00005-08″ style=”position:relative;color:#309b65;cursor:help;border-bottom:1px dotted #309b65;font-weight:bold”>[1] The infection is caused by eating freshwater crustaceans, that is, crabs and crayfish, which carry the infectious form of the parasite. What is specifically dangerous about this disease is that its symptoms are similar to other widespread respiratory illnesses, such as tuberculosis, resulting in its frequent misdiagnosis and delayed treatment.
Paragonimiasis Causative Agent: Paragonimiasis Comprehensive Guide
The infective agents of paragonimiasis are the parasite flatworms of the genus Paragonimus. Researchers have identified over 40 species, and approximately 10 of them cause disease in humans. The clinically significant species are:[2]
- Paragonimus westermani – This is the most widespread cause of human paragonimiasis, the oriental lung fluke, which is mainly found in Southeast Asia and Japan.
- Paragonimus kellicotti – causes epidemics in North America.
- Paragonimus africanus and Paragonimus uterobilateralis– Found in West Africa
- Paragonimus mexicanus -A Parasite that is endemic to Central and South America.
Such worms are reddish-brown and have an oval shape with a length of 7.5 to 12 millimeters and a width of 4 to 6 millimeters. They have two muscular suckers, one at the mouth, called an oral sucker, and one in the middle of the body, called a ventral sucker. Amazingly, even adult flukes may last in the human body up to 20 years and keep producing eggs that result in chronic health conditions.
Life Cycle of Paragonimiasis
The genus Paragonimus lives through a complicated life cycle with more than one host. Knowing this cycle helps explain the spread of the infection and ways of avoiding it.[3]
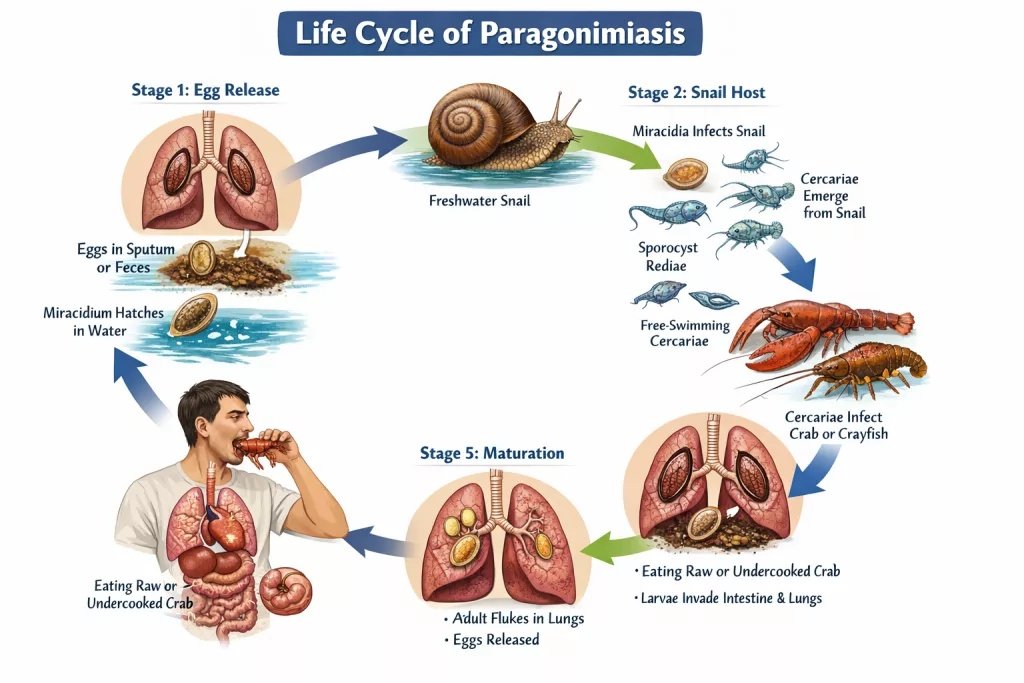
People become infected with Paragonimiasis by eating raw or undercooked crabs or crayfish.
Stage 1: Egg Release
The adult flukes in the lungs of the infected mammals start the cycle by laying eggs. Such eggs get out of the body in coughed sputum or are ingested and released in feces. When the eggs enter freshwater, they hatch to produce small swimming larvae known as miracidia.
Stage 2: Snail Host
The first intermediate host is the freshwater snail, which is actively attacked by the miracidia. The parasites produced inside the snail also have a series of developmental stages- first turning into a sporocyst and then rediae, and lastly generating numerous cercariae. These cercariae hatch after a few weeks out of the snail into the water.
Stage 3: Crustacean Host
The second intermediate host is the crustaceans (crabs or crayfish), which are then invaded by the free-swimming cercariae. In these crustaceans, the parasites attach themselves to tissues and form a metacercaria stage of mammalian infection.
Stage 4: Human Infection
People get infected after consuming raw or undercooked crabs or crayfish with metacercariae. After ingestion, the metacercariae excyst in the duodenum, penetrate the intestinal wall, and migrate through the abdominal cavity.
Stage 5: Maturation
The larvae then penetrate through the diaphragm, pass through the chest cavity, and bore through lung tissue. They enter the airways, where they develop into cysts and become adults after five to six weeks. An adult fluke may live for 20 years in the lungs of a human being, produce eggs, and thus close the cycle.
Symptoms of Paragonimiasis
Symptoms of paragonimiasis depend on the affected organs, as well as the infection stage. Some individuals become asymptomatic and can go on long, and others develop severe complications.[4]
Early Stage Symptoms
The first symptoms appear between 2 and 15 days following the consumption of infected crustaceans when the larvae move through the body. These initial symptoms are diarrhea, stomach aches, and fever. Fatigue, nausea, and general malaise are also some other symptoms that are experienced by some patients at this acute stage. Peripheral eosinophilia is a characteristic laboratory finding during the acute phase.
Chronic Pulmonary Paragonimiasis
The parasites eventually cause respiratory symptoms in weeks to months as they grow up, becoming adults and attacking the lungs.[5]
- A chronic cough that starts with no sputum but gradually turns productive is the most typical symptom.
- Patients produce rusty-coloured or blood-tinged sputum, occasionally coffee-coloured, and with lumps of eggs of the parasites.
- Pain in the chest, especially pleuritic pain which is increased with breathing, is frequent.
- There is shortness of breath and difficulty breathing on exertion.
- There are some patients who develop night sweats, unintended weight loss, and fever.
These lung symptoms are similar to those of tuberculosis, and they are usually misdiagnosed. Some patients may have no noticeable symptoms despite active infection.
Extrapulmonary Symptoms
In other cases, when the parasites move to other body organs, they bring different symptoms.
- Cerebral paragonimiasis (up to 25 percent of hospitalized patients) is a serious but less common manifestation that leads to persistent headaches, seizures, visual impairments, including blurred or double vision, as well as personality changes. Other patients acquire meningitis symptoms, including stiffness of the neck. In around 70 percent of cerebral cases, cognitive decline takes place, and approximately 15 percent go into comas.[6]
- Cutaneous involvement causes migrating subcutaneous lumps or nodules that move beneath the skin.
- Organ-specific symptoms can also develop as a result of the infection of the liver, spleen, intestinal wall, abdominal cavity, and lymph nodes. As a result of a lack of treatment, the flukes are likely to stay longer in the body.
Paragonimiasis Diagnosis
Diagnosis of paragonimiasis may be difficult. The symptoms are similar to other respiratory pathologies, such as tuberculosis or chronic bronchitis. There are a number of ways in which healthcare providers confirm the infection.
Clinical Presentation
The patients usually present with chronic cough, chest pains, and sputum, which is tinged with blood or rusty in colour. Others also have fever, pneumonia, and tiredness. An increase in the number of some white blood cells known as peripheral eosinophilia is a frequent occurrence and can be acute, especially at the initial stages of infection. The clinical appearance tends to resemble tuberculosis, and it is vital to make the diagnosis correctly.
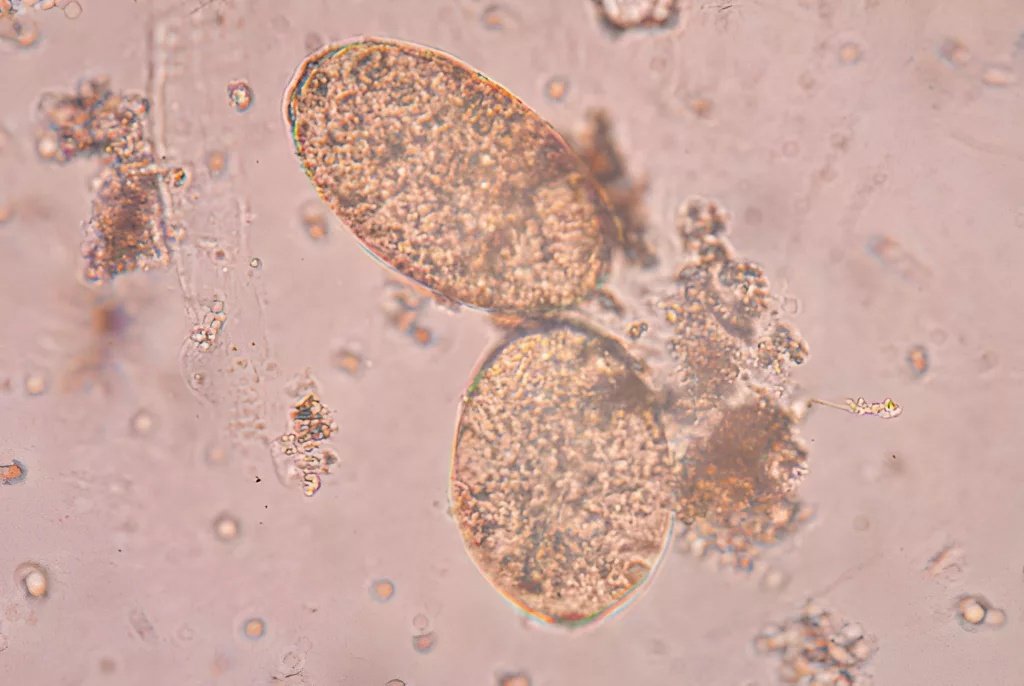
Microscopic Examination
The main diagnosis technique is a microscopic analysis of sputum or stool samples in order to detect Paragonimus eggs. These are oval-shaped, yellowish-brown, and have a characteristic formation like a cap known as an operculum. But eggs do not appear until two or three months after infection. And therefore, it is not possible to diagnose early on using this method. To maximize the chances of detection, several samples of stool on various days should be analyzed through concentration methods. It is worth mentioning that acid-fast staining employed in testing tuberculosis kills the eggs and makes it impossible to diagnose.[7]
Paragonimus westermani is the main parasite responsible for human paragonimiasis.
Serological Testing
Blood tests that show the antibodies of Paragonimus are highly beneficial when eggs are not available or at the earliest stage of infection. Immunoblot tests and enzyme immunoassay tests are sensitive and specific. Such antibody tests are especially useful in diagnosing extrapulmonary infections, i.e, in the brain, where eggs are not excreted in sputum or stool.[8]
Imaging Studies
Chest X-rays and CT scans show several abnormalities such as infiltrates, nodules, cavities, and pleural effusions. One of the typical appearances is known as the “grape cluster” appearance are ring-shaped opacity of interconnected cavities, which is a strong indication of paragonimiasis. In case of possible brain involvement, a brain CT or MRI scan may detect the corresponding grape-like structures, most commonly in the temporal and occipital lobes. Such imaging tests are supportive and do not allow the diagnosis of the infection by themselves.
Differential Diagnosis
Paragonimiasis must be differentiated from several conditions with overlapping symptoms:
| Condition | Key Differentiating Features |
|---|---|
| Tuberculosis | Constitutional symptoms more prominent; acid-fast bacilli in sputum; specific radiographic patterns |
| Lung Cancer | Progressive symptoms, different imaging characteristics, cytology findings |
| Löffler Syndrome | Transient pulmonary infiltrates; different parasitic causes |
| Chronic Obstructive Pulmonary Disease | History of smoking; different pulmonary function tests; no parasitic eggs |
| Fungal Infections | Specific fungal elements on microscopy; different serologic profiles |
Paragonimiasis Treatment
Antiparasitic drugs are effective as a treatment for paragonimiasis. Early intervention is necessary to avoid complications and maintain the treatment up to the end of the infection.
First line Therapy: Praziquantel.
The drug of choice in the treatment of paragonimiasis is praziquantel, which has a very high cure rate of about 80 to 90 percent. The recommended dose is 25 mg per kilogram of body weight by mouth 3 times a day for two days. This drug acts by destroying the outer coating of the parasite, leading to paralysis and death of the flukes. Symptom improvement is very swift, and most of the patients show full recovery of the symptoms, blood abnormalities, as well as changes in the chest X-ray after one to three months.[9]
Alternative Treatment: Triclabendazole
Triclabendazole is a suitable alternative to praziquantel in those regions where the product is not available or when the patient is unable to take it. Patients older than six years should receive the suggested dose of 10 milligrams per kilogram twice, separated by a 12-hour interval. This drug is quite well-tolerated as compared to praziquantel and has cure rates of up to 98.5 percent. Nonetheless, it is not common all over the world, and it might need some special permission from health authorities.[10]
Special Considerations
Where the brain is affected by cerebral paragonimiasis, doctors usually prescribe a steroid course in addition to praziquantel.
These steroids also assist in reducing the inflammatory reaction that happens when the parasites are killed, and the brain continues to swell and get damaged.
Safety Considerations
Both medications are generally well tolerated. Common adverse effects include nausea, headache, dizziness, and abdominal discomfort. Use during pregnancy or breastfeeding should be considered on a case-by-case basis under specialist supervision, where potential benefits outweigh risks.
Follow-up Care
Follow-up tests should be conducted after the treatment to make sure that the infection has disappeared, and they usually include sputum or stool retesting and imaging investigations.
Paragonimiasis Prevention
To prevent paragonimiasis, it is necessary to prevent contact with the parasite by having safe food handling practices and educating people about the disease. The prevention is aimed at interrupting the transmission cycle, as there is no vaccine.[11]
Safe Food Preparation
The best way to prevent this is to make sure that freshwater crustaceans are cooked properly. The Parasitic larvae can only be killed by cooking crabs and crayfish to an internal temperature of at least 145 degrees Fahrenheit or 63 degrees Celsius. Do not eat freshwater crabs or crayfish that are raw, undercooked, pickled, or marinated in wine, as these types of preparation do not kill the infectious metacercariae. This is especially crucial in areas where the cuisine includes eating uncooked or slightly cooked crustaceans.[12]
Kitchen Hygiene
Practice frequent hand washing with warm water and soap when dealing with and cleaning the raw crustaceans. It is necessary to avoid cross-contamination by washing all utensils thoroughly, cutting boards, and serving platters that have been in touch with the raw crustaceans before using them with other foods. Even the little larvae carried by the contaminated surfaces can be infected.
Travel Precautions
Caution is needed by travelers who travel to endemic areas in Asia, Africa, and the western parts of North America and South America. Do not eat traditional dishes that have undercooked freshwater crustaceans, even though they may seem to be cultural delicacies. Take great precautions over the dishes cooked in vinegar or brine, or wine, which are not cooked, because these modes preserve the parasites.
Public Health Education
Education programs in the community are crucial in the endemic areas. The health authorities must educate the people on the risks of transmission with a specific focus on the communities with traditional lifestyles that involve the consumption of raw crustaceans.
Conclusion
Paragonimiasis is a treatable, preventable disease that has been affecting a significant population of millions across the world. Its management is possible by increasing awareness, preparing food correctly, bringing about better sanitation, better diagnostics, and access to treatment. A healthcare professional working in endemic territories should think about paragonimiasis when a patient has chronic respiratory symptoms that are not improving despite receiving treatment against tuberculosis.
The cure is simple: never consume freshwater crabs or crayfish that are raw or undercooked, especially in the endemic areas. Only this practice can get rid of the risk of infection. The work of public health should further focus on education, sanitation, and healthcare infrastructure.
With increased global travel, the awareness of paragonimiasis will need to spread outside the endemic regions. It is possible to mitigate the effects of this disease to a great extent with appropriate prevention and treatment of the condition.
References
[1] Procop GW. North American Paragonimiasis (Caused by Paragonimus kellicotti) in the Context of Global Paragonimiasis. Clin Microbiol Rev. 2009;22(3):415-446. doi:10.1128/CMR.00005-08
[2] Blair D. Paragonimiasis. In: Murrell KD, Fried B, eds. World Class Parasites. Vol 11. Food-Borne Parasitic Zoonoses. New York, NY: Springer; 2007:117-150.
[3] Kim DC. Paragonimus westermani: life cycle, intermediate hosts, transmission to man and geographical distribution in Korea. Arzneimittelforschung. 1984;34(9B):1180-1183.
[4] Im JG, Whang HY, Kim WS, Han MC, Shim YS, Cho SY. Pleuropulmonary paragonimiasis: radiologic findings in 71 patients. Am J Roentgenol. 1992;159(1):39-43.
[5] Choo JD, Suh BS, Lee HS, et al. Chronic pulmonary paragonimiasis: a single-institutional experience with 82 cases. Acta Med Okayama. 2003;57(5):221-228.
[6] Moon JH, Kim HJ, Lee SH, et al. Cerebral paragonimiasis: Clinicoradiological features and serodiagnosis using recombinant yolk ferritin. PLoS Negl Trop Dis. 2022;16(3):e0010240.
[7] Weil GJ, Lane MA, Fischer PU. Serological diagnosis of North American paragonimiasis by Western blot using Paragonimus kellicotti adult worm antigen. Am J Trop Med Hyg. 2013;88(6):1035-1040.
[8] Kong Y, Cho SY, Kang SY, et al. Persisting antibody reaction in paragonimiasis after praziquantel treatment is elicited mainly by egg antigens. Korean J Parasitol. 2002;40(3):131-137.
[9] Chai JY. Praziquantel treatment in trematode and cestode infections: an update. Infect Chemother. 2013;45(1):32-43.
[10] Calvopiña M, Guderian RH, Paredes W, Chico M, Cooper PJ. Treatment of human pulmonary paragonimiasis with triclabendazole: clinical tolerance and drug efficacy. Trans R Soc Trop Med Hyg. 1998;92(5):566-569.
[11] Belizario VY, de Leon WU, Esparar DG, et al. A focus of human infection by Paragonimus westermani in Leyte, the Philippines. Southeast Asian J Trop Med Public Health. 1997;28(Suppl 1):37-45.
[12] Singh TS, Sugiyama H. Epidemiology of paragonimiasis in northeastern India. Indian J Med Res. 2012;136(2):192-204.