
{kind=link}

perianal dermatitis treatment There are some particular kinds of medical conditions that people tend to keep to themselves. Perianal dermatitis, i.e., persistent itching and soreness around the anus, sits squarely in that category. Patients will tolerate it for weeks, sometimes months, before bringing it up with a doctor. This is because they either think it will go away on its own or are too embarrassed.
However, that delay has consequences. Perianal dermatitis is very treatable, but by the time most patients present, they have usually already tried several over-the-counter creams, scratched the area into a worsened state, and occasionally introduced a secondary infection on top of the original problem. Getting the right diagnosis early matters the most.
Another thing to keep in mind is that the term ‘perianal dermatitis’ covers any inflammatory disease of the skin around the anus. It is not really a single diagnosis, but only a presentation of a group of possible causes, and the goal is to try to determine what that cause is. It falls under the category of perianal dermatoses, which in turn fall under the more general categories of skin infection, simple inflammatory conditions, and even generalized skin diseases.
What Is Perianal Dermatitis?
Perianal dermatitis, by definition, is inflammation of the perianal skin, which is the ring of skin immediately surrounding the anal opening. The most common presentation is as anal itching (pruritus ani), but it can also involve soreness, burning, redness, skin thickening, or weeping. In some cases, the skin appears almost normal; in others, it is visibly excoriated, macerated, or lichenified from repeated scratching.
The term pruritus ani is sometimes used interchangeably with perianal dermatitis, but they are not quite the same thing. Pruritus ani is the symptom: anal itching, and perianal dermatitis is the inflammatory process producing it. Not all pruritus ani is dermatitis, and not all perianal dermatitis presents with itch.
The perianal skin is uniquely vulnerable. It is warm, moist, subject to friction, exposed to faecal matter, and covered by some patients with excessive hygiene measures that strip its protective barrier. Any one of these factors can trigger inflammation.
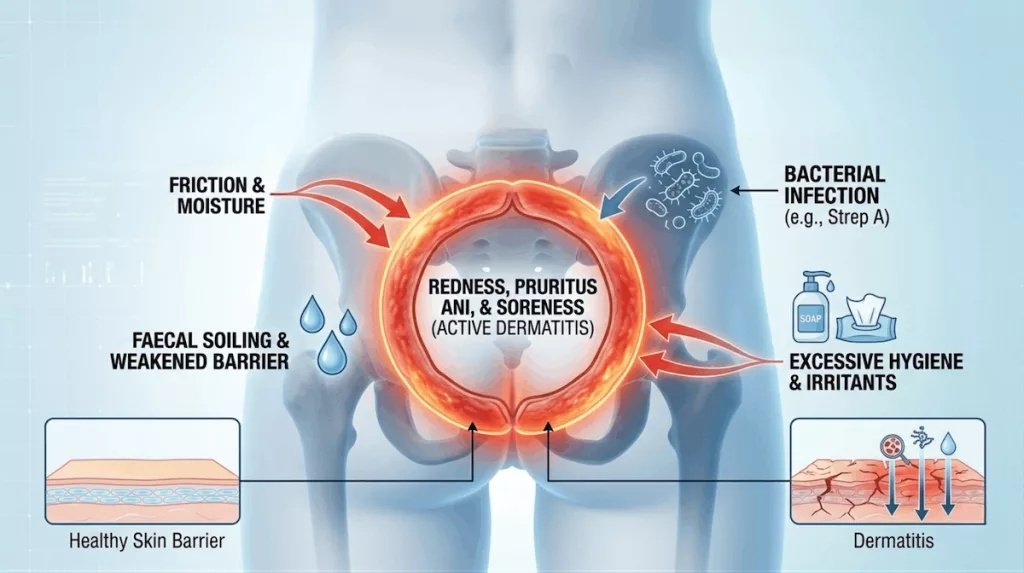
The Perianal Inflammation Roadmap: The factors that can trigger a state of persistent anal itching (pruritus ani) and dermatitis. The intense redness in the center symbolizes the resultinginflammation and active dermatitis. It is the combined endpoint of several distinct drivers: moisture, friction, the disruption of the skin’s barrier by over-cleaning, and the introduction of bacterial or fungal invaders likeStreptococcus or Candida.
What can Cause Perianal Dermatoses?
One of the most important things to understand about perianal dermatitis is that it is not one disease. The presentation: itching, redness, soreness around the anus, is the common endpoint of many different processes. Broadly, the causes fall into the following categories:
| Category | Examples |
|---|---|
| Irritant contact dermatitis | Faecal matter, moisture, over-wiping, soaps, wet wipes, friction |
| Allergic contact dermatitis3Gilissen, L., Schollaert, I., Huygens, S., & Goossens, A. (2021). Iatrogenic allergic contact dermatitis in the (peri)anal and genital area. Contact dermatitis, 84(6), 431–438. | Fragrances, preservatives, topical medications, local anaesthetics (benzocaine, lidocaine), neomycinHSV, HPV, and threadworms (Enterobius vermicularis) are very common and underdiagnosed causes in children |
| Bacterial | Perianal streptococcal dermatitis (especially in children), Staphylococcus aureus |
| Fungal: | Candida albicans, particularly in patients on antibiotics, diabetics, or immunocompromised individuals, dermatophytes (tinea, less common but often missed) |
| Viral or parasitic | Enterobius vermicularis(threadworms, common in children), HSV, HPV (less common but relevant in selected cases) |
| Inflammatory skin disease | Psoriasis, lichen sclerosus, lichen simplex chronicus, seborrhoeic dermatitis |
| Systemic / other | Crohn’s disease, colorectal conditions causing soiling, haemorrhoids, dietary triggers (coffee, spicy food, citrus) |
Irritant dermatitis is the most common cause overall, and in a classic play of paradox, the over-cleaning that patients do in response to symptoms is often what makes it worse instead of improving. The itch-scratch vicious cycle is a major driver of chronicity: scratching worsens the skin barrier, which worsens the itch, which drives more scratching.
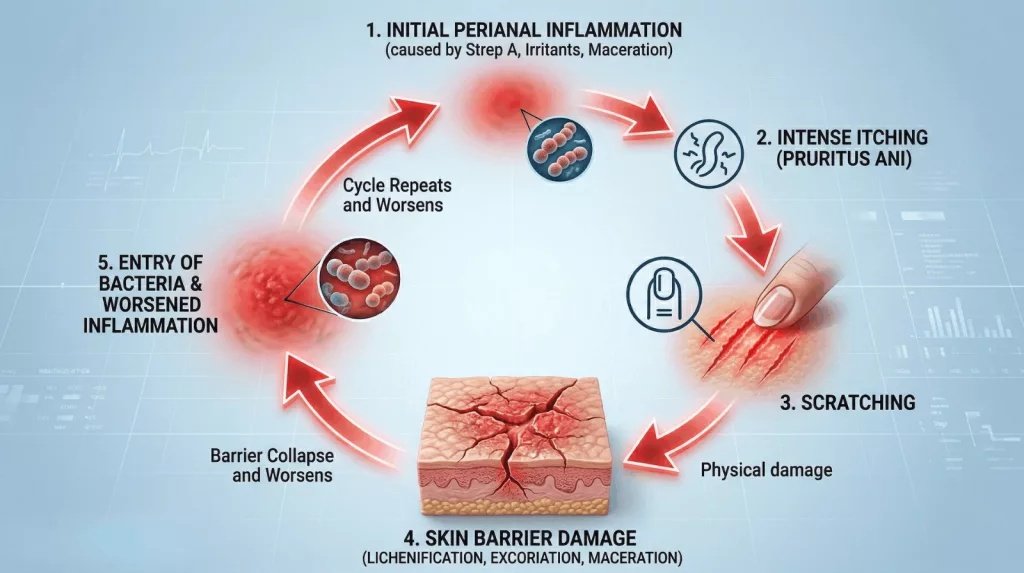
The Itch-Scratch Cycle.The initialPerianal Inflammation(1) creates an intenseItching (Pruritus Ani)(2). Crucially, the simple act ofScratching(3) acts as a physical assault on the already fragileSkin Barrier(4). As seen in the cross-section, this damage collapses the barrier, allowing in more invaders (like bacteria) and increasing metabolic wastes, which directly escalates theInflammation(5) and completes the cycle. Effective treatment must break this cycle, often targeting both the inflammation and the psychological need to scratch.
Perianal Streptococcal Dermatitis
Of all causes of perianal dermatitis, perianal streptococcal dermatitis is probably the most underrecognised, even more so in children, where it is far more common than most clinicians appreciate.
Perianal streptococcal dermatitis is caused by Group A beta-haemolytic Streptococcus (Streptococcus pyogenes), the same bacterium that causes strep throat. The infection presents as a sharply demarcated, bright red rash around the anus, typically without the maceration or satellite lesions you would expect with Candida. The child (or adult) usually complains of pain, itching, and sometimes painful defecation, and parents often report blood-streaked stools.
The condition is frequently missed because it looks like a nappy rash, is attributed to poor hygiene, or simply does not register as an infectious diagnosis. Often, children may be treated repeatedly with antifungal topicals before a clinician thinks about getting a swab of the area.
In adults, perianal streptococcal dermatitis may not be seen as often, but it should always be in the differentials if one sees a very well-defined, bright red perianal eruption that is being treated with conventional antifungal agents and does not resolve.
Recurrence is pretty common, and in some cases, patients may need to go through a longer course of drugs. Some of them may benefit from just getting a throat swab to see if they have accompanying pharyngeal carriage, and they are basically re-infecting themselves because they have the streptococcal throat infection and are not being treated for it.
Symptoms and Clinical Presentation:
Most patients end up going to a doctor once the itching gets so bad that it keeps them up at night. This is made worse by heat, sweating, and certain foods. But the full picture can include:
- Pruritus ani: Intense perianal itching, often nocturnal
- Burning or soreness: Particularly after defecation or in patients who are over-wiping
- Redness and skin changes: Ranging from mild erythema to thickened, lichenified skin in chronic cases
- Weeping or discharge: Suggests maceration, secondary infection, or an underlying condition such as Crohn’s
- Painful defecation or blood on toilet paper: In cases with fissuring
Symptoms that persist beyond a few weeks (or recur across weeks or months) are worth further investigation, rather than trials with empirical treatments. Perianal skin changes may occasionally be the first sign of a more sinister underlying condition: Paget’s disease, Bowen’s disease, and perianal Crohn’s can all have the appearance of simple dermatitis.
Diagnostic Strategies for Perianal Dermatitis
The guideline is to start the diagnosis with a proper history and examination, which sounds obvious, but is often skipped in favour of empirical treatment. History questions to be asked include how long the symptoms have been present, what treatment the patient has already tried, whether there are any bowel symptoms or systemic illness, and, crucially, what the patient’s hygiene habits are like around the area.
Afterwards, the investigations will depend on what direction the clinical suspicion goes, but a complete workup includes:
- Perianal swab for bacterial culture (including specifically requesting Group A Streptococcus) and fungal culture
- Skin scraping: If a fungal infection is suspected clinically
- Patch testing: If allergic contact dermatitis is suspected, particularly in patients using multiple topical products
- Sellotape test or stool microscopy: If threadworms are suspected, particularly in children
- Proctoscopy or colonoscopy: If there are bowel symptoms, bleeding, or the clinical picture raises concern for inflammatory bowel disease or a colorectal cause
- A biopsy is performed if the appearance is atypical, or there is concern for a premalignant or malignant condition
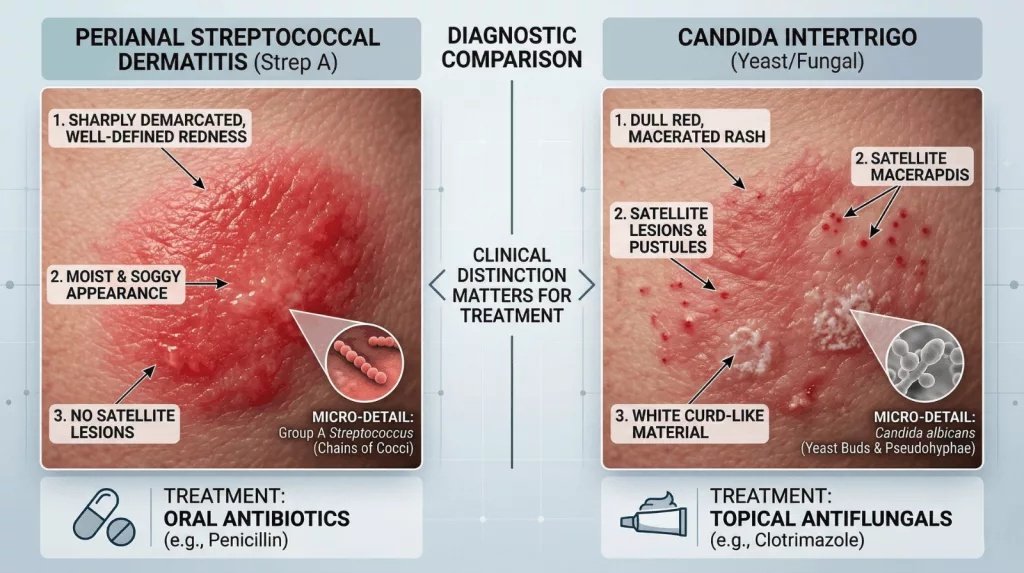
The Critical Diagnostic Comparisonbetween ‘Perianal Streptococcal Dermatitis’ and ‘Candida Intertrigo’, two distinct causes of perianal dermatoses that often overlap in appearance.Streptococcal Dermatitis (Left)is typically abrighter, intenselyred, andsharply demarcatedrash that lacks thesatellite lesions(small red papules, see arrow in right panel) andmaceration(soggy, white appearance) characteristic ofCandida (Right). Recognizing this distinction is critical because treatment differs completely: Strep A requires specific oral antibiotics, while Candida requires targeted topical antifungals.
Perianal Dermatitis Treatment
Treatment has to be directed at the underlying cause, but there are general measures that apply across almost all types.
General Skin Care Measures for all Patients
Even before the cause is established, there are some general hygiene tips and skincare strategies that should be started immediately. These are the foundation of management regardless of cause, and in mild irritant dermatitis, they may be sufficient on their own:
- Gentle cleansing of the area with water only or a fragrance-free soap substitute
- Pat dry rather than rub; some patients benefit from a brief period with a hairdryer on a cool setting
- A barrier cream (zinc oxide or petroleum jelly-based) applied after cleansing to protect the skin
- Loose, breathable cotton underwear
- Avoid dietary triggers if identified: coffee, alcohol, spicy food, and citrus
Treating the Underlying Cause:
Once the cause is established, targeted therapy is started immediately:
- Irritant/allergic contact dermatitis: a short course of mild topical corticosteroid (e.g., 1% hydrocortisone) to settle the inflammation, and removal of the offending agent. Stronger steroids should be used with caution in the perianal area, because there is a high risk of atrophy of this skin.
- Candidal infection: topical antifungal (clotrimazole or miconazole)
- Perianal streptococcal dermatitis: oral penicillin/amoxicillin for 10-14 days; azithromycin in penicillin allergy. Topical treatment alone is not enough.
- Threadworms: single dose of mebendazole or albendazole, repeated after two weeks; all household contacts require treatment at the same time
- Psoriasis/lichen Sclerosus: Dermatology review required; high/moderate potency topical steroids are usually used
- Lichen simplex chronicus: breaking the itch-scratch cycle is the primary goal; potent topical steroids, sedating antihistamines at night, and behavioural measures.
What Not to Do?
There are a few things that can make perianal dermatitis worse, and patients commonly end up doing these by the time they present. The general public should be educated about these.
- Applying topical anaesthetics (lidocaine, benzocaine). These are a common cause of allergic contact dermatitis in this area
- Using steroid-antifungal topical combinations long-term. The steroid component can give quick relief, but ultimately causes atrophy with prolonged use
- Cleaning or repeatedly wiping the perianal area is not as helpful as you would think; instead, it strips the barrier and perpetuates irritation
- Applying multiple over-the-counter (OTC) drugs simultaneously makes it impossible to identify the offending agent if things worsen

This close-up shows lichenification of the back of the knees: skin that has thickened and developed deep ridges as a protective response to months or years of repetitive scratching. Itch-scratch cycle in the perianal area presents a similar picture (Image Courtesy: Salava, A., & Lauerma, A. (2013). Role of the skin microbiome in atopic dermatitis. Clinical and Translational Allergy, 4(1), 33. Available fromWileyand licensed under CC by 4.0)
Prognosis
Most patients with perianal dermatitis will improve as long as the correct diagnosis is made and appropriate treatment is advised. Irritant dermatitis will clear within a few weeks of removing the trigger and establishing good skin care habits. Infections respond well to appropriate antimicrobials. Sometimes the cases drag on untreated, but that is usually because the underlying cause has not been identified, or simply that the itch-scratch cycle cannot be broken.
There are some, such as patients with perianal lichen simplex chronicus, which can be slower to settle. The latter might do better with a dermatology referral rather than repeated trial and observation of empiric treatments in primary care.
Final Words
Perianal dermatitis is a very disruptive condition for the patient, and yet it is not taken seriously enough by the healthcare system. The patients downplay it because it is embarrassing. Clinicians sometimes manage it reflexively with antifungals and move on. Both approaches can do a disservice to the patient.
The range of conditions that fall under perianal dermatoses is wide enough that a proper workup, including swab, history, and examination, is always worth doing. And perianal streptococcal dermatitis in particular is worth keeping front of mind, especially in children: it is common, it is easily confirmed with a swab, and it clears completely with antibiotics. Most of the time, a swab would have given the answer weeks earlier. Nobody thought to do one.
References
[1] Jakubauskas, M., & Dulskas, A. (2023). Evaluation, management and future perspectives of anal pruritus: a narrative review. European journal of medical research, 28(1), 57.
[2] Bender, J. K., Faergemann, J., & Sköld, M. (2017). Skin Health Connected to the Use of Absorbent Hygiene Products: A Review. Dermatology and therapy, 7(3), 319–330.
[3] Gilissen, L., Schollaert, I., Huygens, S., & Goossens, A. (2021). Iatrogenic allergic contact dermatitis in the (peri)anal and genital area. Contact dermatitis, 84(6), 431–438.
[4] Jongen, Johannes M.D.1; Eberstein, Anne M.D.1; Peleikis, Hans-Günter M.D.1; Kahlke, Volker M.D.2; Herbst, Rudolf A. M.D.3. Perianal Streptococcal Dermatitis: An Important Differential Diagnosis in Pediatric Patients. Diseases of the Colon & Rectum 51(5):p 584-587, May 2008.
[5] Van Hemmen Kon, C. L., Brick, L., Valli, B., Marshall, D., Snow, J., Ditchek, J. J., & Schwartz, G. (2025). Perianal Paget’s Disease From Underlying Anal Adenocarcinoma: A Case Study. Cureus, 17(12), e99809.
[6] Burkemper N. M. (2015). Contact Dermatitis, Patch Testing, and Allergen Avoidance. Missouri medicine, 112(4), 296–300.
[7] Pach, S., Nabarro, L., Harris, P., & Eisen, S. (2026). Fifteen-minute consultation: Threadworm in children. Archives of disease in childhood. Education and practice edition, 111(1), 7–10.
[8] Zarrin, N., Rafiei, H., Safari Alamuti, F., Sohrabi, L., & Rashvand, F. (2024). Comparing the efficacy of Zinc Oxide versus Vaseline prophylactic dressings in preventing sacral pressure injuries in patients admitted to the intensive care unit. International wound journal, 21(11), e70139.
[9] Abraham, A., & Roga, G. (2014). Topical steroid-damaged skin. Indian journal of dermatology, 59(5), 456–459.
[10] Wari PK, Dandinavar SF, Amoghimath R, et al. Streptococcal Infections in Children: An Update. Pediatr Inf Dis 2019;1(3):114–119.
[11] Ju, T., Vander Does, A., Mohsin, N., & Yosipovitch, G. (2022). Lichen Simplex Chronicus Itch: An Update. Acta dermato-venereologica, 102, adv00796.
[12] Choi, C., Vafaei-Nodeh, S., Phillips, J., & de Gannes, G. (2021). Approach to allergic contact dermatitis caused by topical medicaments. Canadian family physician Medecin de famille canadien, 67(6), 414–419.