
{kind=link}

Warfarin Toxicity Signs Warfarin toxicity is a condition that occurs due to an excessive amount of warfarin or related vitamin-K antagonists in the body, leading to an increased risk of bleeding. Severe cases can cause life-threatening hemorrhage and require prompt reversal and supportive care.
Warfarin, also known by its brand name Coumadin, is a vitamin K antagonist. It is the most common oral anticoagulant used for the prevention and treatment of thromboembolic disease. Its broad-ranging applications in the treatment of individuals with dilated cardiomyopathy, pulmonary embolism, venous thrombosis, chronic atrial fibrillation, and mechanical heart valves have led to widespread exposure to this drug. Long-acting “superwarfarins” (rodenticide compounds such as brodifacoum) produce much more prolonged coagulopathy and require prolonged therapy.
Chemical Structure of Warfarin
Etiology of Warfarin Toxicity: Warfarin Toxicity Signs
Warfarin was initially used as a pesticide and later formulated as a medication. Toxicity can occur due to various reasons. These include intentional, unintentional, and pediatric ingestion.
- Intentional overdose in Adults: Intentional overdose is the most obvious cause. However, it is relatively rare. A 25-year survey of two tertiary centres reported only a total of 22 non-pediatric intentional overdoses.
- Unintentional overdose: Unintentional toxicity is more common and may occur during initial dosing, due to changes in diet, drug–drug interactions (e.g., with antibiotics, antifungals, amiodarone, or trimethoprim-sulfamethoxazole), impaired liver function, or metastatic liver disease. Genetic polymorphisms in CYP2C9 and VKORC1 also influence patient susceptibility to over-anticoagulation.
- Pediatric ingestion: In children, toxicity usually results from accidental exploratory ingestion.
Pathophysiology of Warfarin Toxicity
The pathophysiology of warfarin toxicity centres on its mechanism of action as a vitamin K antagonist. Vitamin K epoxide reductase enzyme is essential for recycling vitamin K in the liver. Warfarin and superwarfarins primarily act through inhibition of 2,3-vitamin K epoxide reductase and cause a deficiency of active vitamin K.
This deficiency leaves the II, VII, IX, X coagulation factors and proteins S and C inactive. By blocking the vitamin K recycling, warfarin reduces the synthesis of fully functional clotting factors. Hence, it impairs the blood coagulation cascade and increases the risk of bleeding. In acute overdose or chronic excessive dosing, this inhibition is exaggerated, producing profound deficiencies of clotting factors and a severe risk of hemorrhage.
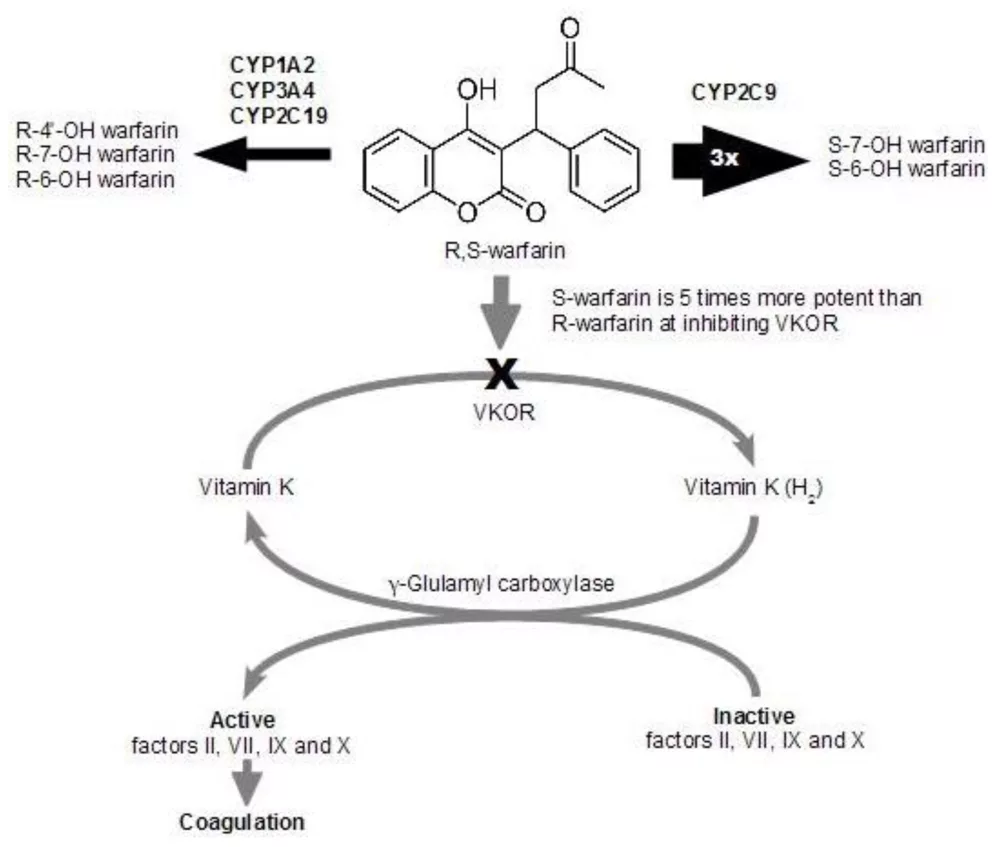
Warfarin metabolism. (Warfarin is metabolized in the liver. CYP1A1, CYP1A2, and CYP3A4 metabolize the (R)-enantiomer, and CYP2C9 metabolizes the more potent (S)-enantiomer. Warfarin inhibits vitamin K reductase complex subunit 1 to interfere with the vitamin-K-dependent carboxylation of clotting factors prothrombin II, VII, IX, and X. Image Courtesy: Warfarin Toxicity and Individual Variability—Clinical Case by Piatkov et al. 2010, doi.org/10.3390/toxins2112584, available via: https://www.mdpi.com/2072-6651/2/11/2584#, CC BY 4.0.
Toxicokinetics of Warfarin Toxicity
After oral ingestion, warfarin is quickly absorbed through the gastrointestinal tract. However, INR elevation is usually delayed and may not be seen for 12–24 hours, with the peak effect occurring at 36–72 hours because of the half-lives of clotting factors. Warfarin’s anticoagulant effect can last several days. Superwarfarins, in contrast, have extremely long half-lives and may cause prolonged coagulopathy for weeks to months, requiring extended vitamin K therapy
Symptoms of Warfarin Toxicity
Symptoms of warfarin toxicity revolve primarily around bleeding due to excessive anticoagulation, and they range from mild to severe. Some cases can also be asymptomatic. These symptoms include:
- Severe headache
- Dizziness
- Severe stomach pain
- Abdominal discomfort
- Bleeding gums
- Nose Bleeds
- Unexplained bruising
- Heavy and prolonged bleeding from even small cuts or injuries
- Blood in urine (Hematuria)
- Black or bloody stools
- Increased menstrual bleeding
- Vomiting blood
- Signs of internal bleeding (such as intracranial hemorrhage or gastrointestinal bleeding)
Rare but severe complications include warfarin-induced skin necrosis. Warfarin toxicity can also cause symptoms of anemia, weakness, or fatigue due to blood loss.
Doctors recommend low-molecular-weight heparin or unfractionated heparin as anticoagulants in pregnant women.
Warfarin Toxicity During Pregnancy
Warfarin use is generally contraindicated in pregnancy as its toxicity during pregnancy poses significant risks to both mother and fetus.
Warfarin crosses the placenta due to its low molecular weight. It inhibits vitamin K-dependent synthesis of clotting factors and bone growth proteins in the fetus. The critical period for teratogenic effects is mainly in the first trimester. However, bleeding complications can occur throughout pregnancy. The toxicity can cause fetal warfarin syndrome if exposure happens in the first trimester. This syndrome is characterized by:
- Growth retardation
- Skeletal abnormalities
- Nasal hypoplasia
- Stippled epiphyses
Exposure to warfarin during the later stages of pregnancy can cause:
- Seizures
- Fetal bleeding
- Hydrocephalus
- Stillbirth or miscarriage
Some other malformations associated with warfarin toxicity are:
- Eye anomalies
- Congenital heart defects
- Limb hypoplasia
- Hearing loss
- Midline central nervous system defects
- Developmental delays
In pregnant women requiring anticoagulation, low-molecular-weight heparin is the preferred alternative.
Diagnosis of Warfarin Toxicity
Diagnosis starts with the physical examination and the history of the patient.
Physical & History
Physical examination includes assessment of signs and symptoms indicative of bleeding, such as bruising, nose bleeding, dark urine or stools, mucosal bleeding, or gastrointestinal bleeding.
The healthcare provider asks about the following things:
- What type of medication did you ingest?
- Any concurrent ingestions, such as alcohol or drugs?
- What medicines are you taking currently?
- Timing and intention of warfarin?
- Do you have any recent history of trauma, especially to the head?
- Do you have any underlying medical conditions?
Laboratory Tests
Laboratory tests assess complete blood count, international normalized ratio, prothrombin time, basic metabolic, liver function tests, and others.
International Normalized Ratio (INR) Prothrombin Time (PT)
INR is the gold standard for warfarin effect assessment, as an elevated INR and prolonged PT confirm impaired coagulation of the patient. INR is the gold standard for assessing warfarin effect. A therapeutic INR is usually 2.0–3.0 (2.5–3.5 in mechanical valves); values >3.0 suggest increased risk, and an INR >10 without bleeding warrants vitamin K therapy.
Complete Blood Count (CBC)
CBC assesses for anemia from blood loss. It also monitors platelet counts to rule out thrombocytopenia.
Partial Thromboplastin Time (PTT)
PTT can also be prolonged, but it can be less specific than PT/INR.
Fibrinogen Level
They are usually normal in warfarin toxicity, but they help rule out some coagulation disorders like disseminated intravascular coagulation.
Basic Metabolic Panel
Basic metabolic and liver function tests evaluate metabolism and comorbidities.
Additional Diagnostic Test
Blood type and crossmatch are necessary if significant bleeding is suspected and transfusion is anticipated. Additionally, CT or MRI is warranted if intracranial bleeding is suspected; abdominal imaging can assess for retroperitoneal hemorrhage.
Treatment & Management of Warfarin Toxicity
Treatment and management depend on the severity of bleeding and levels of anticoagulation. The first step is to cease further ingestion of warfarin immediately.
Asymptomatic Patients without Bleeding
- Avoid PCC or FFP unless bleeding develops.
- Hold one or more doses of warfarin.
- If INR >10 without bleeding, give oral vitamin K (2.5–5 mg).
Intentional Ingestion in Non-anticoagulated Patients
- Intentional ingestion, regardless of reported doses, requires serial INR monitoring.
- Vitamin K is only administered if the INR exceeds 10 or bleeding occurs.
Patients with Active Bleeding
These patients require emergent reversal of warfarin-induced coagulopathy. The cornerstone of the treatment in such patients includes:
- 4F-PCC (Four-Factor Prothrombin Complex Concentrate) is the preferred option because it can rapidly normalize INR within minutes. However, it carries a small but real risk of thromboembolism. The recommended intravenous dose is 50 IU/kg (maximum 5,000 IU).
- If 4F-PCC is not available, the doctor may use 3F-PCC in combination with Fresh Frozen Plasma (FFP) (150–300 mL, or 10–15 mL/kg) to replace factor VII, which is lacking in 3F-PCC. When FFP is used alone, the dose is 15 mL/kg, adjusted for INR level and patient weight.
- Intravenous vitamin K (10 mg infused slowly over 30 minutes) should be administered to restore endogenous synthesis of vitamin K-dependent clotting factors. It is worth noting that providers usually avoid subcutaneous administration because of unreliable absorption.
- In case of surgical or mucosal bleeding, tranexamic acid (an antifibrinolytic agent) can be used adjunctively. It can promote hemostasis.
- Plasma transfusion is the key option when PCC is contraindicated or unavailable. It is the best option, especially for patients with intracranial hemorrhage (when rapid INR reversal is very critical). The recommended dose is 15 to 30 mL/kg. This dose can achieve 30 to 50% of normal clotting factor levels.
- As a last resort in severe, refractory bleeding when PCC and FFP are unavailable or ineffective, your doctor may alternatively consider Recombinant Activated Factor VII (rFVIIa). It can provide rapid hemostasis but carries a high risk of thromboembolic complications, so its use is limited and should be reserved for life-threatening situations.
Pediatric and superwarfarin cases
- Superwarfarins often require prolonged high-dose oral vitamin K with frequent INR checks.
- The doctor may also recommend Vitamin K prophylaxis depending on the dose.
Supportive Care
Supportive care includes management of shock and organ dysfunction caused by the bleeding and monitoring vital signs and coagulation parameters closely.
Differential Diagnosis
The differential diagnosis of warfarin toxicity includes:
- Child abuse, especially in pediatric patients with bruising.
- Epistaxis(the first sign of coagulopathy that can be trauma-induced or spontaneous).
- Postpartum hemorrhage
- Ectopic pregnancy
- Gastrointestinal bleeding
- Subarachnoid or subdural hemorrhage
- Vitreous hemorrhage (Bleeding into the eye that may cause visual changes)
- Type A and B hemophilia (Inherited coagulation disorders presenting with prolonged bleeding due to deficiencies of factor VIII or IX, which can mimic excessive anticoagulation)
- Munchausen syndrome (A factitious disorder where patients deliberately feign or induce symptoms, such as bleeding, to assume the sick role.)
- Hypovolemic shock
Final Review
Warfarin, which was initially marketed as a rodenticide, has been used as a medicine for more than half a century. Toxicity occurs when an excessive amount accumulates in the body. Clinicians should educate the patients about drug–drug interactions, consistent vitamin K intake, and the importance of INR monitoring. Pharmacists and clinicians must ensure other medications do not adversely interact with warfarin. Warfarin toxicity usually requires admission to the hospital, and the outcomes of the treatment depend on the presence of bleeding.
References
[1] Deaton, J.G. and T.M. Nappe, Warfarin toxicity. 2017.
[2] Carpenter M, Berry H, Pelletier AL. Clinically Relevant Drug-Drug Interactions in Primary Care. Am Fam Physician. 2019 May 01;99(9):558-564.
[3] Deaton, J.G. and T.M. Nappe, Warfarin toxicity. 2017.
[4] Erdoğan, M., et al., Epidemiological features of warfarin overdose and efficacy of prothrombin complex concentrates. Journal of Experimental and Clinical Medicine, 2013. 30(4): p. 327-330.
[5] Schwalfenberg, G.K., Vitamins K1 and K2: the emerging group of vitamins required for human health. Journal of nutrition and metabolism, 2017. 2017(1): p. 6254836.
[6] Deaton, J.G. and T.M. Nappe, Warfarin toxicity. 2017.
[7] Toyoda, K., Antithrombotic therapy for pregnant women. Neurologia medico-chirurgica, 2013. 53(8): p. 526-530.
[8] Abadi, S., A. Einarson, and G. Koren, Use of warfarin during pregnancy. Canadian Family Physician, 2002. 48(4): p. 695-697.
[9] Conway, S.E., et al., Laboratory and clinical monitoring of direct-acting oral anticoagulants: what clinicians need to know. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy, 2017. 37(2): p. 236-248.
[10] Long, N., Warfarin toxicity. Toxicology, 2020.
[11] Long, N., Warfarin toxicity. Toxicology, 2020.
[12] Karunarathna, I., et al., Warfarin Toxicity: Mechanisms, Clinical Manifestations, and Management.
[13] Karunarathna, I., et al., Warfarin Toxicity: Mechanisms, Clinical Manifestations, and Management.
[14] Long, N., Warfarin toxicity. Toxicology, 2020.
[15] Ansari, A. M., Khorasanchi, A., Faghihimehr, A., & Toor, A. (2021). Recombinant activated factor VII in a patient with intracranial hemorrhage and severe thrombocytopenia.Clinical Case Reports,9(10), e04788. https://doi.org/10.1002/ccr3.4788