
{kind=link}

Serotonin Syndrome Symptoms Serotonin syndrome is a potentially life-threatening drug reaction caused by excessive serotonergic activity in the central nervous system. It most often occurs due to therapeutic medication use, drug interactions, recreational substances, or intentional overdose. Serotonin is a neurotransmitter which is produced naturally in the body but can also be found in certain medications, supplements, and some other substances. Serotonin syndrome can occur in all ages without any sex preference, and its incidence is difficult to measure due to its uncommon, mild, and unfamiliarity of the condition.
The clinical severity of the condition varies from mild to fatal, and symptoms include neuromuscular excitation, autonomic dysfunction, and altered mental dysfunction.[1] Prevention includes careful monitoring of medication use and avoidance of the use of multiple serotonin-increasing drugs. The primary treatment options involve the discontinuation of the offending medications.
What Causes Serotonin Syndrome? : Serotonin Syndrome Symptoms
The main cause of serotonin syndrome is excessive stimulation of serotonin receptors, usually due to elevated synaptic serotonin in the central nervous system. Brain nerve cells, the spinal cord, and the intestine are responsible for producing serotonin, which assists in controlling the mood, behaviour, body temperature, attention, digestive processes, breathing, and blood circulation. While a single serotonergic drug can sometimes precipitate the syndrome, it most often occurs when multiple medications that increase serotonin are combined, or in cases of intentional or accidental overdose.
For example, an overdose of antidepressants may cause serotonin syndrome, but the condition is also seen when an antidepressant is taken together with an opioid pain medication. Certain dietary supplements and illicit drugs such as ecstasy (MDMA), cocaine, and amphetamines can also be responsible.
The drugs and supplements that may possibly cause this syndrome include:
Pain Medications:
Pain medications that can affect the serotonin level of the body include:
- Tramadol
- Meperidine
- Fentanyl
- Methadone
- Oxycodone, hydrocodone, and codeine (rarely, and usually when combined with other serotonergic drugs)
Anti-Migraine Medications:
These include triptans such as:
- Sumatriptan
- Naratriptan
- Almotriptan
Antidepressants:
Three classes of antidepressants can cause serotonin syndrome. These antidepressants include:
Tricyclic Antidepressants
These include:
- Clomipramine
- Amitriptyline
- Desipramine
- Nortriptyline
- Imipramine
- Trimipramine
- Doxepin
Selective Serotonin Reuptake Inhibitors (SSRIs)
This group of antidepressants includes:
- Escitalopram
- Citalopram
- Sertraline
- Fluvoxamine
- Paroxetine
- Fluoxetine
Serotonin & Norepinephrine Reuptake Inhibitors (SNRIs)
This group of antidepressants includes:
- Levomilnacipran
- Duloxetine
- Venlafaxine
- Milnacipran
- desvenlafaxine
Other antidepressants include:
- Monoamine oxidase inhibitors (phenelzine and isocarboxazid)
- Norepinephrine reuptake inhibitors (bupropion)
- Serotonin modulators (trazodone and nefazodone).
Other Medications:
Some other medications that might play a role in causing the disease are:
- Cough medicine (dextromethorphan)
- Anti-nausea medications (metoclopramide, ondansetron, droperidol)
- Antibiotics (linezolid)
- Antiretroviral medications (ritonavir).
Pathophysiology of Serotonin Syndrome
Serotonin (5-hydroxytryptamine or 5-HT) functions as a biochemical mediator both centrally and peripherally and is involved in various complex physiological processes.
The peripheral actions of serotonin involve:
- Platelet aggregation
- Gastrointestinal motility
- Bronchoconstriction
- Uterine contraction
- Vasoconstriction[2]
In the central nervous system, it is present in the raphe nuclei of the brainstem. Here, it inhibits excitatory neurotransmission and modulates:
- Emesis
- Motor tone
- Thermoregulation
- Appetite
- Mood
- Attention
Many drugs have been developed to manipulate the concentrations of serotonin in the body and the syndrome arises when there is an excessive stimulation of serotonin receptors in both the peripheral and central nervous systems. These receptors get triggered by the drugs that elevate the synaptic serotonin levels. The serotonin binds to multiple families of 5-HT. No single receptor is responsible for this syndrome; the subtypes 5-HT1A and 5-HT2A play a significant role.[3]
Importantly, symptoms usually develop within hours of exposure or dose adjustment of a serotonergic drug, which helps distinguish serotonin syndrome from conditions such as neuroleptic malignant syndrome, where onset is slower.
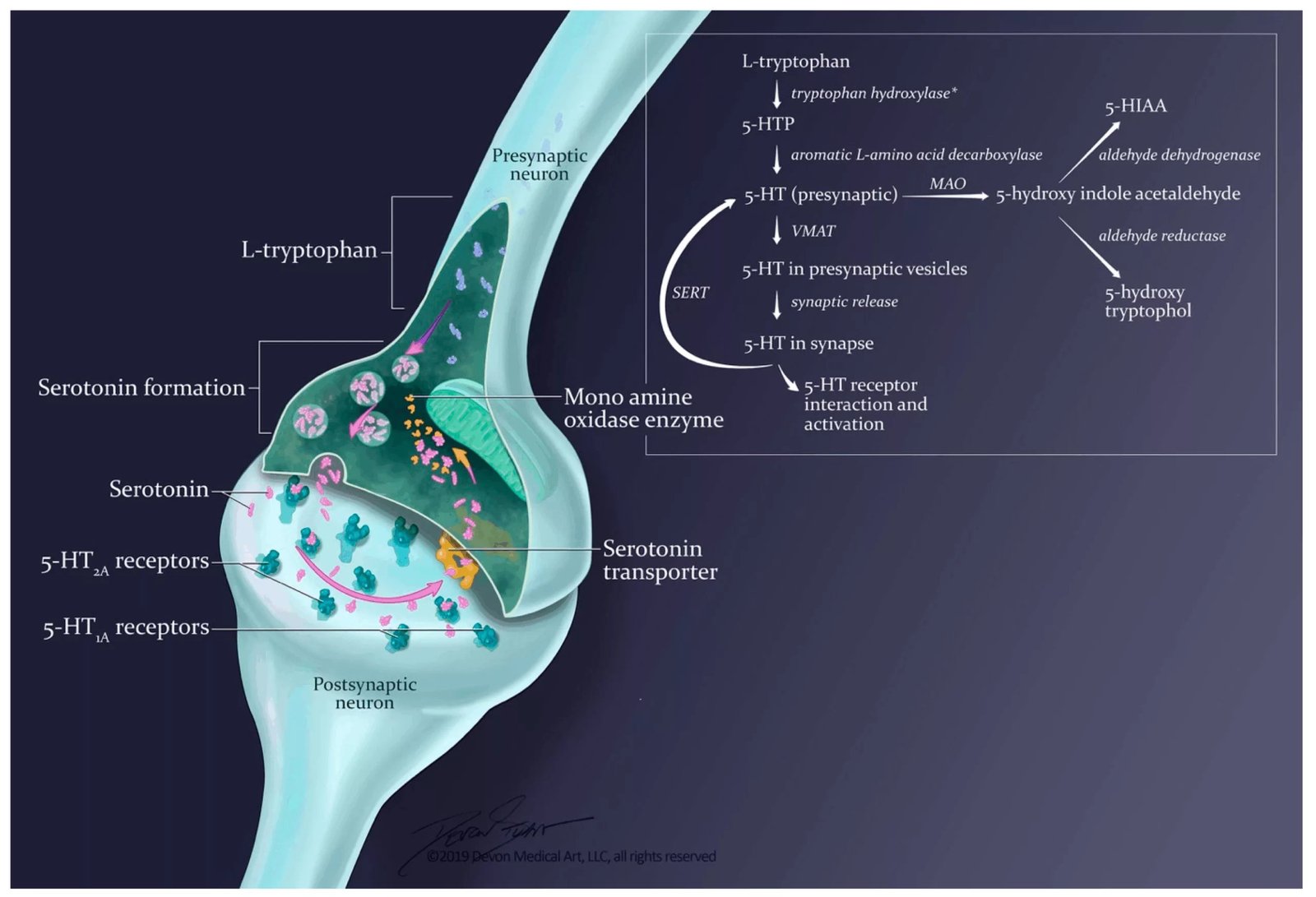
Normal serotonergic neurons. Image courtesy: The Serotonin Syndrome: From Molecular Mechanisms to Clinical Practice by Francescangeli et al, 2019, doi.org/10.3390/ijms20092288, available via https://www.mdpi.com/1422-0067/20/9/2288, CC BY 4.0.
Symptoms of Serotonin Syndrome
The severity of the condition varies from mild to severe, and the common symptoms of this syndrome include:
- Restlessness
- Agitation
- High blood pressure
- Rapid heart rate
- Confusion
- Ocular clonus (abnormal rhythmic eye movements)
- Loss of muscle coordination
- Muscle rigidity
- Twitching muscles
- Muscle spasms
- Tremor
- Dilated pupils
- Goosebumps
- Shivering
- Headache
- Diarrhea
- Heavy sweating
- Disorientation
- Delirium
- High body temperature
- Seizures
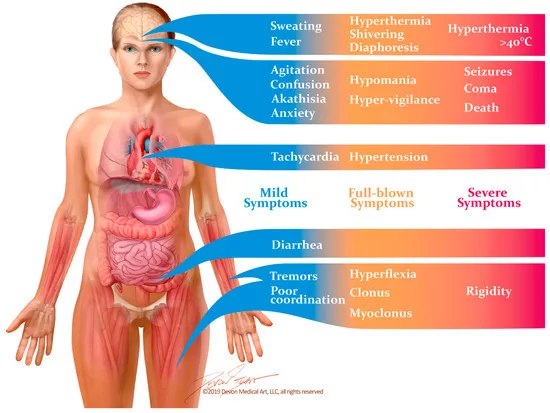
Signs and symptoms of the serotonin syndrome occur along a spectrum of severity. Image Courtesy: The Serotonin Syndrome: From Molecular Mechanisms to Clinical Practice by Francescangeli et al, 2019, doi.org/10.3390/ijms20092288, available via https://www.mdpi.com/1422-0067/20/9/2288, CC BY 4.0.
Diagnosis of Serotonin Syndrome
The diagnosis is clinical. Several diagnostic criteria exist, with the Hunter Toxicity Criteria being the most accurate. A detailed medical history and medication review are essential, as serotonin syndrome usually appears within hours (typically <12h) of starting, increasing, or combining serotonergic drugs.
History & Physical Examination:
The healthcare provider obtains a detailed history of medications, illicit substances, and supplements upon suspicion of serotonin syndrome. In addition to the name of the substance, doses, and schedules, information related to the changes in medication or administration of new substances is also crucial. Onset of symptoms and their rate of progression are essential in diagnosing the condition. Serotonin syndrome symptoms usually appear within 6 to 12 hours of intake of a serotonergic agent or a change in its dose.[4]
It can be challenging to obtain a patient’s history if the patient had an altered mental state, which is the most common symptom of this syndrome. Physical examination plays a key role, as the syndrome is often identified by its characteristic triad of symptoms: neuromuscular hyperactivity (such as tremor, clonus, or hyperreflexia), autonomic instability (fever, high blood pressure, rapid heart rate, or sweating), and changes in mental status (ranging from agitation to confusion or coma).
Laboratory Evaluations:
To clarify the clinical picture and assessment of the severity of the syndrome, laboratory evaluations can assist. The common non-specific laboratory findings include:
- Elevated white blood cell count
- Elevated creatine phosphokinase
- Decreased sodium bicarbonate
In severe serotonin syndrome, the laboratory findings include:
- Platelet abnormalities
- Intravascular coagulation
- Elevated creatine kinase CK
- Metabolic acidosis
- Rhabdomyolsis
Hunter Toxicity Diagnostic Criteria:
There are several diagnostic criteria, such as Sternbach, Radomski, and Hunter. Hunter criteria are the most accepted and accurate ones with 97% specificity and 84% sensitivity.[5]
Following is the list of Hunter Toxicity Criteria Decision Rules
A diagnosis is made in a patient with recent serotonergic drug exposure plus one of the following findings:
- Hyperreflexia and tremor
- Spontaneous clonus
- Ocular clonus with diaphoresis (excessive sweating) and agitation
- Inducible clonus with diaphoresis and agitation
- Hypertonia and temperature above 38 °C with ocular or inducible clonus
Management or Treatment of the Serotonin Syndrome
Management and treatment of serotonin syndrome include immediate cessation of serotonergic agents, supportive therapy, and serotonin antagonists.
Cessation of Serotonergic Agents:
Discontinuing all serotonergic agents is the first step in treating the condition. As serotonin syndrome is a toxicity, the syndrome resolves with the removal of the offending agents. However, some serotonergic agents (such as fluoxetine) have long half-lives, hence the symptoms can also persist for multiple days.[6]
Supportive Therapy:
Supportive care after cessation of the serotonergic agents can normalize the vital signs. It includes:
- Administration of intravenous fluids and oxygen
- Intravenous crystalloids to treat volume depletion in hyperthermia
- Continuous cardiac and vital sign monitoring
- Correction of autonomic instability (abnormal blood pressure or heart rate)
Management of Autonomic Instability:
For hypertension or tachycardia, short-acting agents such as nitroprusside, nicardipine, or esmolol are recommended.[7] To treat hypotension, the recommended direct-acting sympathomimetic agents are:
- Epinephrine
- Norepinephrine
- Phenylephrine
Sedation:
Doctors highly recommend chemical restraints (sedation) in serotonin syndrome, as the condition causes delirious agitation with muscle contraction, which significantly contributes to hyperthermia and elevation of creatine kinase. Physical restraints are avoided to manage the condition as they can cause significant muscle contraction and worsen the condition. Benzodiazepines are preferred for sedation as they can assist in controlling tachycardia and high blood pressure.
Serotonin Antagonists:
If chemical sedation, management of vital signs and supportive measures do not adequately treat the serotonin syndrome, then an antidote is the next management step. Cyproheptadine has non-specific 5-HT1A and 5-HT2A antagonistic properties. The initial recommended dose of this antagonist is 12 mg, and 2 mg is administered every 2 hours.A maintenance dose of 8 mg is given every 6 hours once stabilized.[8]
Prognosis of Serotonin Syndrome
The prognosis relies on the severity of the serotonin toxicity. Mild cases often resolve within 24–72 hours after discontinuation of the offending drug, while severe cases require intensive care. After treatment and resolution of the syndrome, a comprehensive assessment is required to assess the risks and benefits of continuing the previous serotonergic regimen.
Complications of Serotonin Syndrome
If left unmanaged, serotonin syndrome can progress to life-threatening complications, including:
- Seizures
- Severe hyperthermia
- Respiratory failure
- Rhabdomyolysis
- Unconsciousness or coma
- Death
Serotonin Syndrome vs Neuroleptic Malignant Syndrome (NMS)
Serotonin syndrome and NMS are both life-threatening conditions with overlapping symptoms. However, they differ in certain features, which are summarized in Table 1.
Table 1: Key Differences between Serotonin Syndrome versus NMS
| Features | Serotonin Syndrome | NMS |
|---|---|---|
| Causative agent | Serotonergic drugs | Dopamine antagonists |
| Onset | Rapid | Slow |
| Mental state | Altered, agitation, and coma. | Stupor, variable, can be coma or alert. |
| Treatment | Withdrawal of the offensive agent, supportive care, sedation, and antagonists. | Withdrawal of the offensive agent, supportive care, and dantrolene, etc. |
Final Remarks
Serotonin syndrome is a drug-induced syndrome. It results from increased serotonin activity. The disease may progress via an overdose, intoxication or a combined effect of serotonergic agent that causes an increase in serotonergic effects. The Hunter Serotonin Toxicity Criteria are the most widely accepted and accurate diagnostic criteria for serotonin syndrome. Due to the widespread use of serotonergic drugs, there is a high clinical suspicion for this syndrome. Morbidity and mortality can be avoided by early diagnosis and therapy.
References
[1] Duma, S.R. and V.S. Fung, Drug-induced movement disorders. Australian prescriber, 2019. 42(2): p. 56.
[2] Berger, M., J.A. Gray, and B.L. Roth, The expanded biology of serotonin. Annual review of medicine, 2009. 60(1): p. 355-366.
[3] Celada, P., et al., The therapeutic role of 5-HT1A and 5-HT2A receptors in depression. Journal of psychiatry and neuroscience, 2004. 29(4): p. 252-265.
[4] Ramsay, R.R., C. Dunford, and P. Gillman, Methylene blue and serotonin toxicity: inhibition of monoamine oxidase A (MAO A) confirms a theoretical prediction. British journal of pharmacology, 2007. 152(6): p. 946-951.
[5] Dunkley, E., et al., The Hunter Serotonin Toxicity Criteria: simple and accurate diagnostic decision rules for serotonin toxicity. Qjm, 2003. 96(9): p. 635-642.
[6] Martin, T.G., Serotonin syndrome. Annals of Emergency Medicine, 1996. 28(5): p. 520-526.
[7] Boyer, E.W. and M. Shannon, The serotonin syndrome. New England Journal of Medicine, 2005. 352(11): p. 1112-1120.
[8] Scotton, W.J., et al., Serotonin syndrome: pathophysiology, clinical features, management, and potential future directions. International Journal of Tryptophan Research, 2019. 12: p. 1178646919873925.