
{kind=link}

What is Sporotrichosis?: Sporotrichosis Symptoms Treatment
Sporotrichosis Symptoms Treatment Sporotrichosis, also known as rose handler’s disease,is a fungal infection that may be localised to the skin, lungs, bones, and joints, or become systemic. Sporotrichosis is caused by fungi of the Sporothrix schenckii species complex. Its exact incubation period remains unknown and may range from a few days to a few months, the average being 3 weeks.
How Does It Present?
Clinically, it presents with firm, painless nodules that later ulcerate. Sporotrichosis occurs in three main clinical types: lymphocutaneous, fixed cutaneous, and disseminated cutaneous or extracutaneous sporotrichosis. Extracutaneous or systemic sporotrichosis occurs from hematogenous spread from the primary inoculation site. In children, the clinical profile is almost similar, but facial involvement is more frequent.
Who Is at Risk of Sporotrichosis?
Sporotrichosis is a subcutaneous fungal infection that is present worldwide and is common in tropical and subtropical areas. In particular, rose gardeners, farmers, miners, horticulturists, and armadillo hunters have an increased risk of infection. The condition usually occurs in individuals working in agriculture or with plants and plant materials. In animals, infected cats are a major zoonotic source of transmission.
Life Cycle of Sporotrichosis: How the Infection Develops?
Sporotrichosis is a severe fungal infection that occurs following traumatic inoculation through cuts or abrasions, either due to working with rose plants or in soil, or from cats’ paws. It affects both people and animals, irrespective of age and gender. The traumatic inoculation of the fungus on the exposed surfaces of the skin is the most common route of the infection; the upper limbs are affected twice as commonly as the lower limbs.
Disease Progression: Stages of Sporotrichosis Infection
Sporotrichosis does not occur overnight; instead, it develops through a sequence of pathogenic events, and the first lesion usually appears after at least 20 days
Saprophytic or Mould Phase:
In this phase, the fungus is in spore form and is present in the environment, on plants, in the soil, or on the cats.
Traumatic Inoculation or Inhalation Phase:
The spores of the fungus then enter the human body (or any animal body) by either traumatic exposure through cuts and scratches or, rarely, by inhalation while working with affected plants.
Yeast Phase:
In the host body, these spores then convert themselves into yeast or an active form that causes the symptoms.
Lymphatic/ Hematogenous Spread Phase:
The fungal cells then spread along the lymphatic system throughout the body, forming papules and nodules on the skin.
Systemic Phase:
Other than affecting the skin, sometimes the fungus also affects bones and joints and may spread to the lungs, causing serious complications and even death.
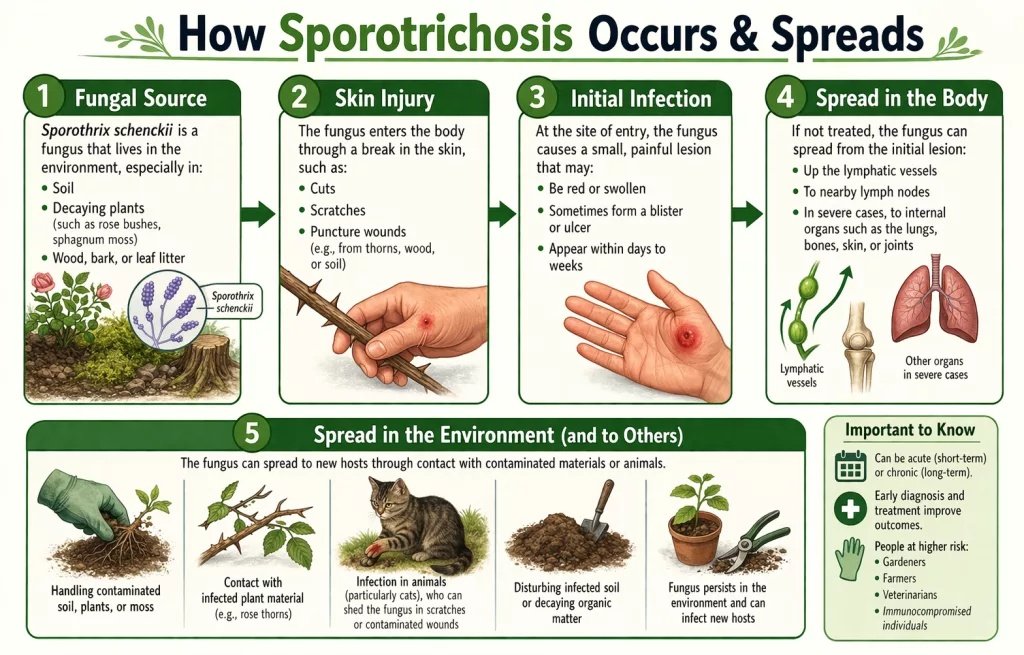
The image explains the spread of Sporotrichosis.
Early and Common Symptoms
The signs and symptoms of sporotrichosis are both cutaneous and extracutaneous. Nearly 80% of the affected patients present the lymphocutaneous form.
Skin Lesions and Their Progression
Initially, the lesion has a papulonodular appearance on the skin, appearing between two and four weeks after the trauma (the first nodule appearing at about the 20th day). Afterwards, the lesion may ulcerate and form draining sinuses. This is known as the inoculation chancre. The lesions, usually nodules, follow the path along the regional lymphatic channels; depending on the anatomical site, in both upward and downward directions, after some weeks.
Effect on Eyes
The ocular mucosa is more commonly involved, causing conjunctivitis, episcleritis, uveitis, choroiditis, and retrobulbar lesions.The simultaneous affection of the ocular mucosa and the regional lymph nodes is one of the causes of the Parinaud Oculoglandular Syndrome, a condition most commonly associated with cat scratch diseasebut also seen in infections like sporotrichosis.
Bones and Joints Involvement
Bones and joints become involved either through direct invasion from an overlying cutaneous lesion following trauma or indirectly through hematogenous spread. Osteoarticular sporotrichosis is a disease that includes monoarthritis, with or without any overlying cutaneous lesion, but has bone resorption and osteolytic lesions in the most severe cases.
Effect on Lungs
In the lungs, inhalation of spores directly or the hematogenous spread of spores indirectly causes the disease. It is more common in immunosuppressed patients presenting with the disseminated systemic form of sporotrichosis. The signs and symptoms may include coughing, dyspnea, hemoptysis, etc, depending on the type and site involved. Radiologic images, such as chest radiography or computerized tomography, are important in making the diagnosis.
Is Sporotrichosis Contagious?
Sporotrichosis is not contagious, as person-to-person transmission is extremely rare. But it spreads from animals to human beings.
Certain factors are responsible for its broad spectrum, like the mode of transmission and spread, the size and depth of the traumatic part of the skin, the host’s immunity, and the virulence and thermotolerance of the fungus.
How Is Sporotrichosis Diagnosed?
Sporotrichosis can be diagnosed through a combination of clinical and laboratory investigations. Definitive diagnosis relies on laboratory confirmation of Sporothrix species, along with supportive clinical findings. The infection can be confirmed using culture, cytopathology, histopathology, serology, and molecular techniques..
Moreover, complementary laboratory tests such as RBC count, WBC count, and biochemical parameters may be required in systemic cases.
Mycological Culture (Gold Standard)
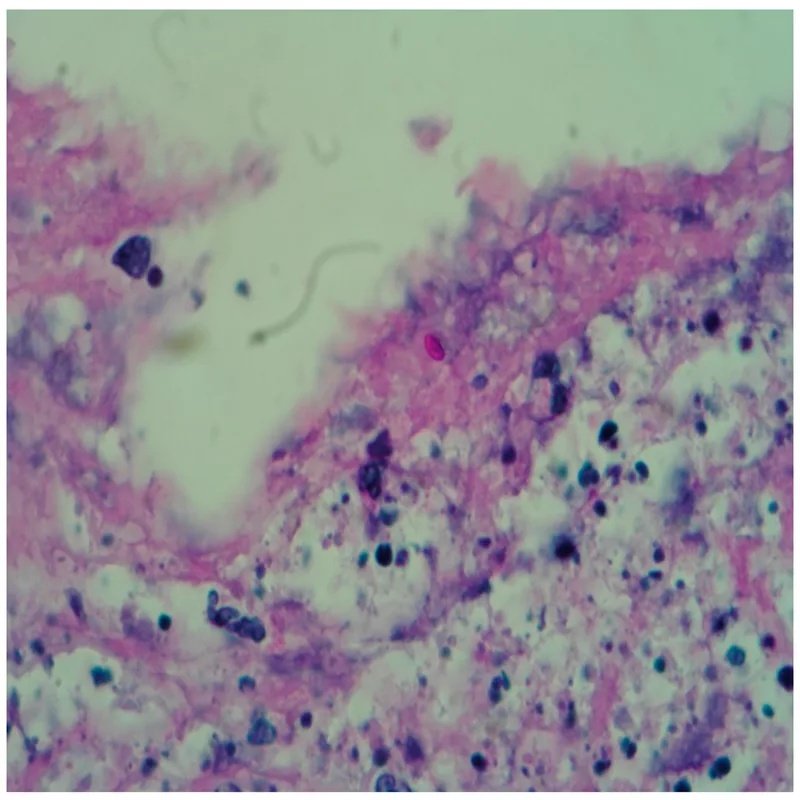
The gold standard for the diagnosis of sporotrichosis is the isolation and identification of the Sporothrix species from clinical samples of skin lesions, aspirates from floating abscesses, as well as other body fluids, including blood and cerebrospinal fluid. It is a simple and low-cost diagnostic method, although it may not be useful for some systemic and atypical forms of sporotrichosis.
Under a magnification of 375X, this photomicrograph of a mouse tissue specimen showed a number of Sporotrichum sp. yeast cells, while one of the cells in the center was undergoing the reproductive process known as budding, which would lead to the creation of genetically identical duplicated yeast cells. The image is taken from theCDCsite and is an open-access image.
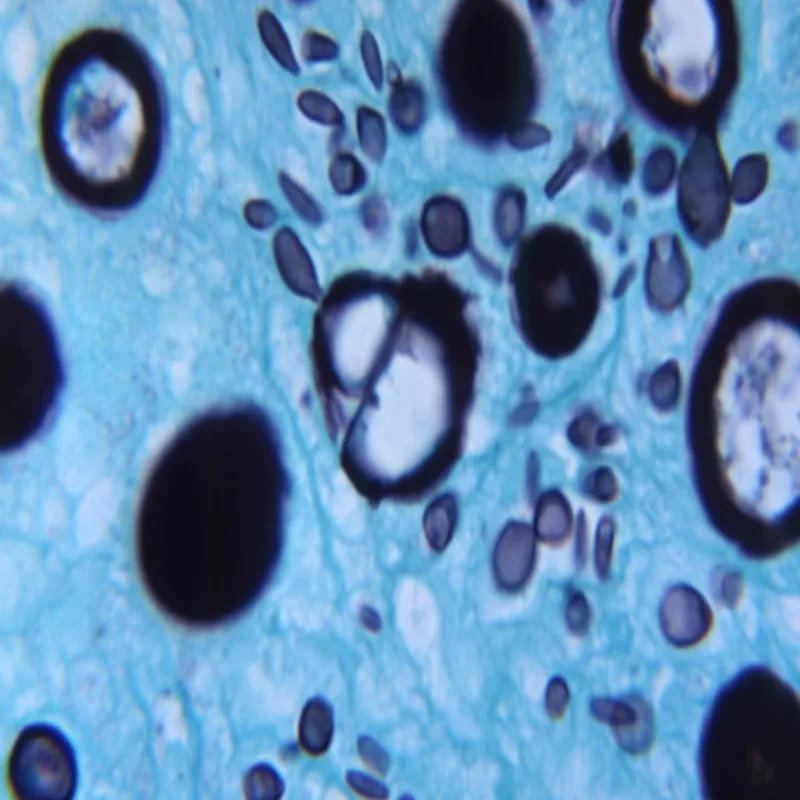
Microscopy, Cytology, and Histopathology
The inflammatory infiltrate can be observed by hematoxylin-eosin stain. PAS or methenamine silver is used to identify the fungal structures. The sensitivity of these tests is low.
Skin biopsy stained with PAS in which yeast can be observed (40×). This image is taken from theMDPIwebsite and is licensed under the CC BY license.
Serological Testing
Serological ELISA test using the SsCBF (Sporothrix schenckii Con A-Binding Fraction) is an efficient method for the detection of IgG antibodies in the serum of patients with cutaneous sporotrichosis. While useful as supportive evidence, serology has variable sensitivity and specificity depending on the clinical form of the disease.
Molecular Diagnosis (PCR-Based Methods)
The polymerase chain reaction (PCR) and its variants (Species-Specific PCR, Rolling Circle Amplification) are widely used in the diagnosis of sporotrichosis.
Treatment Options for Sporotrichosis
The treatment choice for sporotrichosis depends on the disease’s symptoms, the host’s immunity, and the species of Sporothrix involved. The most virulent species (S. brasiliensis, S schenckii, and S. globosa) exhibit different responses to different antifungals. Management options include pharmacological therapy and, in selected cases, non-pharmacological interventions.
Topical Therapy
Topical treatment has a limited role in sporotrichosis and is generally not effective as monotherapy. It is not considered a standard primary treatment option for established infection.
Oral Antifungal Therapy
Oral drugs for the treatment of Sporotrichosis are:
Potassium Iodide Solution
KI saturated solution has been used for treating sporotrichosis since 1903. However, its use has declined due to poor tolerability and frequent side effects, although it may still be used in selected settings.
Itraconazole:
Itraconazole is considered the drug of choice due to its effectiveness. It is a fungistatic drug that acts by inhibiting ergosterol synthesis, which is essential for fungal cell membrane integrity.
Itraconazole started to be used in sporotrichosis treatment in the late 1980s. Its therapeutic dose may range from 100 to 400 mg/day, depending upon the severity of the disease. For children weighing up to 20 kg, the dose of itraconazole is 5 to 10 mg/kg/day. Although it is very effective, it has some potential side effects like headaches, gastrointestinal upset, hepatotoxicity, and teratogenicity. The contraindications for its use include pregnancy and patients with liver problems.
Terbinafine:
Terbinafine is considered an alternative antifungal agent in some cases of cutaneous sporotrichosis. It is generally well tolerated, but its safety in pregnancy is not fully established, so it should be used with caution.
Intravenous Amphotericin B
IV amphotericin B is reserved for severe, disseminated, or life-threatening sporotrichosis, particularly in immunocompromised patients or those with pulmonary, osteoarticular, or systemic involvement.
Non-Pharmacological Treatment
Non-pharmacological measures are also effective in treating sporotrichosis, and they include cryosurgery and thermotherapy.
Cryosurgery:
Cryosurgery may be used as an adjunct treatment, especially in localized chronic lesions that respond poorly to antifungal therapy.
Thermotherapy:
Local hyperthermia (local heat therapy) and cryosurgery are safe and effective options for treating pregnant women with cutaneous sporotrichosis. It is a safer alternative to antifungals or can be used in combination with them.
Surgical Management
Surgical intervention is not routinely required, but may be considered in selected cases, such as localized pulmonary disease or refractory lesions not responding to medical therapy.
Emerging and Adjunct Therapies
Photodynamic therapy has shown promising results in early studies, but it is still considered experimental. Further clinical evidence is needed before it becomes part of standard management.
Prevention of Sporotrichosis
General prevention is to wear gloves, long sleeves, heavy boots, and masks while working with plants or handling the animals (especially cats).
In areas where cats are mainly responsible for the disease, the application of certain policies regarding their proper hygiene and wellness can prevent the spread of this disease.
Conclusion:
In short, Sporotrichosis is a subcutaneous fungal infection that can range from mild cutaneous disease to severe systemic involvement, caused by Sporothrix species found in soil, plants, and animals. The treatment depends on the stage at which the disease is diagnosed. Although it is curable and most cases resolve within 3-6 months of the therapy, severe systemic infection can be life-threatening. Proper preventative measures, while working in the soil or handling the animals, can help reduce the disease.
References
[1] Proia, Laurie (2020). “28. The dimorphic mycoses”. In Spec, Andrej; Escota, Gerome V.; Chrisler, Courtney; Davies, Bethany (eds.).Comprehensive Review of Infectious Diseases. Elsevier. pp. 421–422.
[2] Johnstone, Ronald B. (2017). “25. Mycoses and Algal Infections”.Weedon’s Skin Pathology Essentials(2nd ed.). Elsevier. p. 455.
[3] López-Romero, Everardo; et al. (2010). “Sporothrix schenckii complex and sporotrichosis, an emerging health problem”.Future Microbiology. 6 (1): 85–102.
[4] Mercurio M. G. and Elewski B. E., Therapy of sporotrichosis,Seminars in Dermatology. (1993) 12, no. 4, 285–289, 2-s2.0-0027139771.
[5] James, William D.; Elston, Dirk; Treat, James R.; Rosenbach, Misha A.; Neuhaus, Isaac (2019). “13. Diseases resulting from fungi and yeasts”.Andrews’ Diseases of the Skin: Clinical Dermatology(13th ed.). Elsevier. pp. 314–315.
[6] Bonifaz A., Saúl A., Paredes-Solis V. et al., Sporotrichosis in childhood: clinical and therapeutic experience in 25 patients,Pediatric Dermatology. (2007) 24, no. 4, 369–372,
[7] Rodrigues AM, Gonçalves SS, de Carvalho JA, Borba-Santos LP, Rozental S, Camargo ZP. Current Progress on Epidemiology, Diagnosis, and Treatment of Sporotrichosis and Their Future Trends. J Fungi (Basel). 2022 Jul 26;8(8)
[8] Mahajan V. K., Sharma N. L., Sharma R. C., Gupta M. L., Garg G., and Kanga A. K., Cutaneous sporotrichosis in Himachal Pradesh, India,Mycoses. (2005) 48, no. 1, 25–31
[9] da Rosa A. C. M., Scroferneker M. L., Vettorato R., Gervini R. L., Vettorato G., and Weber A., Epidemiology of sporotrichosis: a study of 304 cases in Brazil,Journal of the American Academy of Dermatology. (2005) 52, no. 3, 451–459,
[10] Barros MB, Schubach AO, Schubach TM, Wanke B, Lambert-Passos SR. An epidemic of sporotrichosis in Rio de Janeiro, Brazil: epidemiological aspects of a series of cases. Epidemiol Infect. 2008;136:1192-6
[11] Lopes-Bezerra LM, Schubach A, Costa RO. Sporothrix schenckii and sporotrichosis. An Acad Bras Cienc. 2006;78:293-308.
[12] Curi AL, Félix S, Azevedo KM, Estrela R, Villar EG, Saraça G. Retinal granuloma caused by Sporothrix schenckii. Am J Ophthalmol. 2003;136:205-7.
[13] Ferreira CP, Nery JA, de Almeida AC, Ferreira LC, Corte-Real S, Conceição-Silva F. Parinaud’s oculoglandular syndrome associated with Sporothrix schenckii. IDCases. 2014;1:38-9.
[14] Costa RO, de Mesquita KC, Damasco PS, Bernardes-Engemann AR, Dias CM, Silva IC, et al. Infectious arthritis as the single manifestation of sporotrichosis: serology from serum and synovial fluid samples as an aid to diagnosis. Rev Iberoam Micol. 2008;25:54-6.
[15] Orofino-Costa R, Unterstell N, Carlos Gripp A, de Macedo PM, Brota A, Dias E, et al. Pulmonary cavitation and skin lesions mimicking tuberculosis in a HIV negative patient caused by Sporothrix brasiliensis. Med Mycol Case Rep. 2013;2:65-71
[16] Kwon-Chung K. J., Comparison of isolates ofSporothrix schenckiiobtained from fixed cutaneous lesions with isolates from other types of lesions,Journal of Infectious Diseases. (1979) 139, no. 4, 424–431, 2-s2.0-0018395065
[17] Barros, M.B.; de Almeida Paes, R.; Schubach, A.O.Sporothrix schenckiiand sporotrichosis.Clin. Microbiol. Rev.2011,24, 633–654.
[18] Rodrigues, A.M.; Della Terra, P.P.; Gremiao, I.D.; Pereira, S.A.; Orofino-Costa, R.; de Camargo, Z.P. The threat of emerging and re-emerging pathogenicSporothrixspecies.Mycopathologia2020,185, 813–842 Marimon, R.; Cano, J.; Gené, J.; Sutton, D.A.; Kawasaki, M.; Guarro, J.Sporothrix brasiliensis,S. globosa, andS. mexicana, three newSporothrixspecies of clinical interest.J. Clin. Microbiol.2007,45, 3198–3206.
[19] Orofino-Costa, R.C.; Macedo, P.M.; Rodrigues, A.M.; Bernardes-Engemann, A.R. Sporotrichosis: An update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics.An. Bras. De Dermatol.2017,92, 606–620
[20] Morris-Jones R. Sporotrichosis. Clin Exp Dermatol. 2002;27:427-31.
[21] Hessler C, Kauffman CA, Chow FC. The Upside of Bias: A Case of Chronic Meningitis Due to Sporothrix schenckii in an Immunocompetent Host. Neurohospitalist. 2017;7:30-4
[22] Penha CV, Bezerra LM. Concanavalin A-binding cell wall antigens of Sporothrix schenckii: a serological study. Med Mycol. 2000;38:1-7. fungal cell components are imporatant in makin the diagnosis.
[23] Hu, S.; Chung, W.-H.; Hung, S.-I.; Ho, H.-C.; Wang, Z.-W.; Chen, C.-H.; Lu, S.-C.; Kuo, T.-T.; Hong, H.-S. Detection ofSporothrix schenckiiin clinical samples by a nested PCR assay.J. Clin. Microbiol.2003,41, 1414–1418.
[24] Espinel-Ingroff, A.; Abreu, D.P.B.; Almeida-Paes, R.; Brilhante, R.S.N.; Chakrabarti, A.; Chowdhary, A.; Hagen, F.; Cordoba, S.; Gonzalez, G.M.; Govender, N.P.; et al. Multicenter and international study of MIC/MEC distributions for definition of epidemiological cutoff values (ECVs) for species ofSporothrixidentified by molecular methods.Antimicrob. Agents Chemother.2017,61, e01057-17.
[25] Orofino-Costa, R.C.; Macedo, P.M.; Rodrigues, A.M.; Bernardes-Engemann, A.R. Sporotrichosis: An update on epidemiology, etiopathogenesis, laboratory and clinical therapeutics.An. Bras. De Dermatol.2017,92, 606–620.Sharma B, Sharma AK, Sharma U. Sporotrichosis: a Comprehensive Review on Recent Drug-Based Therapeutics and Management. Curr Dermatol Rep. 2022;11(2):110-119.
[26] de Lima Barros MB, Schubach AO, de Vasconcellos Carvalhaes de Oliveira R, Martins EB, Teixeira JL, Wanke B. Treatment of cutaneous sporotrichosis with itraconazol-study of 645 patients. Clin Infect Dis. 2011;52:e200-6.Barros MB, de Almeida Paes R, Schubach AO. Sporothrix schenckii and Sporotrichosis. Clin Microbiol Rev. 2011 Oct;24(4):633-54.
[27] de Lima Barros, M.B.; Schubach, A.O.; de Vasconcellos Carvalhaes de Oliveira, R.; Martins, E.B.; Teixeira, J.L.; Wanke, B. Treatment of cutaneous sporotrichosis with Itraconazole—Study of 645 patients.Clin. Infect. Dis.2011,52, e200–e206.
[28] Fichman, V.; Valle, A.C.F.d.; de Macedo, P.M.; Freitas, D.F.S.; Oliveira, M.M.E.d.; Almeida-Paes, R.; Gutierrez-Galhardo, M.C.
[29] Ferreira, C.P.; do Valle, A.C.; Freitas, D.F.; Reis, R.; Galhardo, M.C. Pregnancy during a sporotrichosis epidemic in Rio de Janeiro, Brazil.Int. J. Gynaecol. Obs.2012,117, 294–295.
[30] Legabão, B.C.; Fernandes, J.A.; de Oliveira Barbosa, G.F.; Bonfim-Mendonça, P.S.; Svidzinski, T.I.E. The zoonosis sporotrichosis can be successfully treated by photodynamic therapy: A scoping review.Acta Trop.2022,228, 106341.