
{kind=link}

Impetigo Symptoms Treatment Impetigo is a common infection among children living in hot and humid climates. The disease can manifest as both bullous and non-bullous. The infection usually occurs on the face but can also occur on any other part of the body with an abrasion, laceration, insect bite, or trauma.
What is Impetigo?: Impetigo Symptoms Treatment
Impetigo is a highly contagious bacterial infection of the skin that affects the epidermis, the outermost layer of the skin. It is most commonly caused by Staphylococcus aureus and, less commonly, Streptococcus pyogenes (group A Streptococcus). The condition usually presents as red sores or blisters that rupture and form characteristic honey-colored crusts. The infection spreads easily through close physical contact or by sharing contaminated items such as towels, clothing, and bedding.
Nonbullous impetigo is the most common form and accounts for nearly 70% of cases. Although impetigo mainly affects children between the ages of two and five years, adults can also develop the infection, particularly in crowded environments or after skin injury.
What Causes Impetigo?
The two main bacteria that cause impetigo are Staphylococcus aureus and Streptococcus pyogenes. These bacteria enter through breaks in the skin, including cuts, scratches, insect bites, burns, eczema, or other irritated areas.
The infection does not look the same in everyone. Depending on the bacterial strain and the toxins produced, impetigo may appear as nonbullous lesions with crusting or as bullous lesions with large fluid-filled blisters.
Some individuals are more vulnerable to infection than others. Risk factors include:
- Hot and humid climates
- Crowded living conditions
- Poor hygiene
- Close-contact sports
- Daycare or school exposure
- Skin conditions such as eczema or scabies
- Diabetes or weakened immune systems
It is also important to note that Impetigo can also spread from one area of the body to another through scratching, a process known as autoinoculation.
Incubation Period for Impetigo
The incubation period of impetigo depends on the bacteria causing the infection.
- Streptococcal impetigo usually develops within 1–3 days after exposure.
- Staphylococcal impetigo typically develops within 4–10 days.
A person may spread the infection even before obvious symptoms appear. Close contact with infected individuals is the most significant risk factor for transmission.
Types of Impetigo
There are a few different types of impetigo, including non-bullous, bullous and ecthyma.
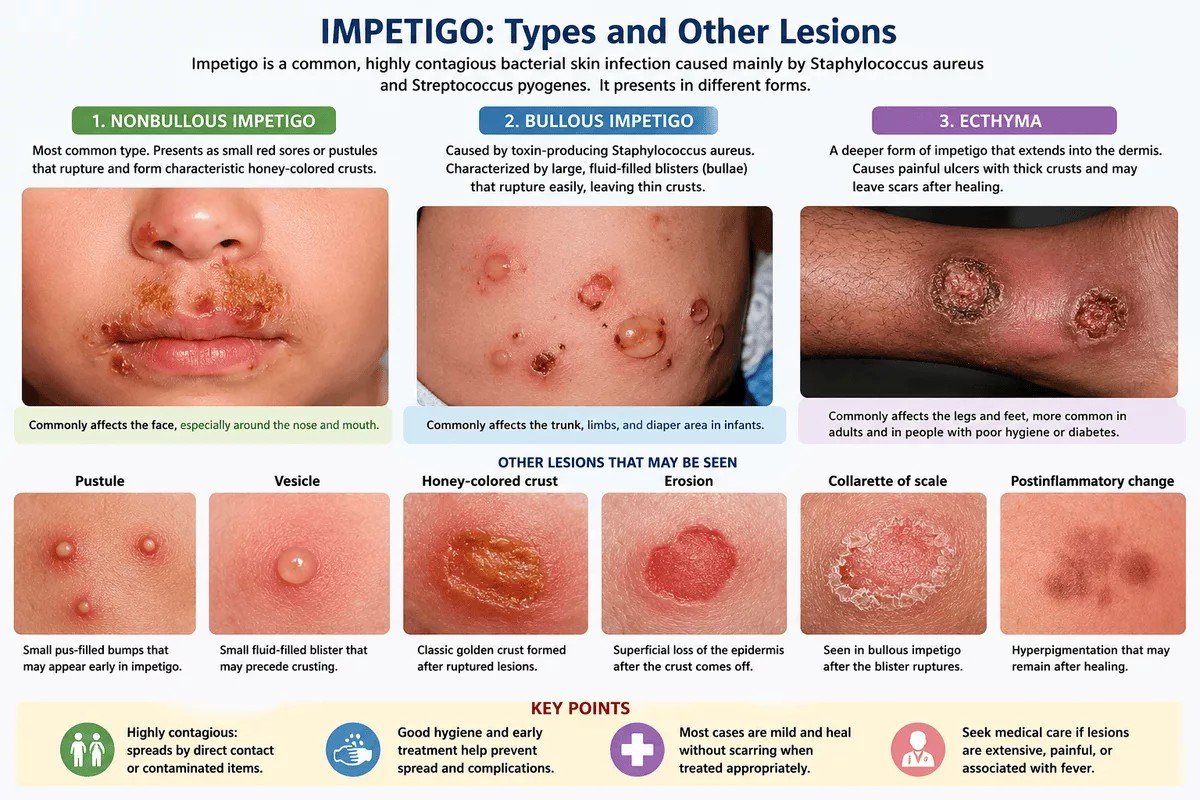
Visual overview of impetigo types and associated skin lesions, including nonbullous impetigo, bullous impetigo, and ecthyma, with characteristic clinical features such as honey-colored crusting and blistering.
Impetigo Contagiosa (Nonbullous impetigo)
Impetigo contagiosa is the most common form of impetigo. It is an acute, superficial skin infection characterized by small vesicles or pustules that rupture and form thick, honey-colored crusts. The lesions commonly occur on the face, especially around the nose and mouth, but may also involve the neck, arms, legs, or trunk.
The condition is usually caused by Staphylococcus aureus, although Streptococcus pyogenes may also be involved. The lesions are highly contagious but generally heal without scarring when properly treated.
Bullous impetigo:
Bullous impetigo is caused exclusively by toxin-producing strains of Staphylococcus aureus. It is characterized by large, fragile, fluid-filled blisters called bullae. These blisters rupture easily and leave behind thin brown crusts and a collarette of scale around the edges.
Bullous impetigo commonly affects infants and young children. The lesions are usually found on the trunk, extremities, axillae, and diaper region. Systemic symptoms are uncommon but may include fever, weakness, or diarrhea in severe cases. The condition generally resolves within two to three weeks without scarring.

Fluid-filled bullae on the leg
Ecthyma
Ecthyma is a deeper and more severe form of impetigo that extends into the dermis. It produces painful ulcers covered with thick crusts and may leave scars after healing. The lesions commonly affect the legs and feet and are more likely to occur in individuals with poor hygiene, diabetes, or weakened immunity.
Symptoms of Impetigo
Although the appearance of lesions varies between bullous and nonbullous impetigo, both forms usually begin with superficial skin sores that spread easily through scratching or close contact.
Impetigo typically starts as small red sores or blisters that rupture and release fluid or pus. Within a few days, the lesions form the characteristic honey-colored crusts associated with the infection.
The sores most commonly appear around the nose and mouth but may also affect the arms, legs, hands, trunk, or other exposed areas of the body. The lesions may itch or cause mild discomfort.
Nonbullous impetigo usually causes smaller crusted lesions, whereas bullous impetigo produces larger fluid-filled blisters that rupture easily. Bullous lesions are more commonly seen on the trunk, diaper area, and skin folds.
Swollen lymph nodes near the infected skin may occur in some patients. Fever and other systemic symptoms are uncommon but may develop in more severe infections.
Scratching the lesions can spread the bacteria to other areas of the body (Autoinoculation).

Bullous impetigo on the chin showing ruptured blisters and yellow crusting.Image Credit: Photo by James Heilman, MD, via Wikimedia Commons (CC BY-SA 4.0)
How is Impetigo Diagnosed?
Nonbullous and bullous impetigo are usually diagnosed clinically based on their appearance. The characteristic honey-colored crusts often make the diagnosis straightforward.
Skin swabs are not routinely necessary because they may not distinguish bacterial colonization from active infection. However, culturing pus or fluid from bullae may be useful in recurrent cases, severe infections, or when first-line treatment fails. This helps identify the causative bacteria and determine antibiotic sensitivity.
The differential diagnosis includes herpes simplex infection, contact dermatitis, eczema, scabies, candidiasis, varicella, and erysipelas.
| Condition | How it Differs from Impetigo |
|---|---|
| Herpes simplex | Painful grouped blisters rather than honey-colored crusts |
| Eczema | Dry, inflamed, itchy patches without bacterial crusting |
| Contact dermatitis | Triggered by irritants or allergens with prominent itching |
| Scabies | Intensely itchy rash with burrows, especially between fingers |
| Varicella (Chickenpox) | Widespread itchy vesicles in different stages of healing |
| Erysipelas | Deeper skin infection with sharply raised red borders and fever |
| Candidiasis | Moist red rash commonly affecting skin folds |
| Insect bites | Localized itchy bumps without typical honey-colored crusts |
Impetigo Complications
Impetigo is usually mild, but complications can occasionally occur, particularly when the infection is untreated or severe. Possible complications include:
- Cellulitis
- Lymphangitis
- Abscess formation
- Post-streptococcal glomerulonephritis
- Rarely, sepsis
Post-streptococcal glomerulonephritisis a rare kidney complication that may develop after Streptococcus pyogenes infection. Symptoms may include swelling, dark urine, and high blood pressure.
Treatment of Impetigo:
The goals of treatment are to relieve discomfort, improve the appearance of lesions, prevent the spread of infection, and reduce the risk of recurrence.
Topical Treatment
Localized impetigo is usually treated with topical antibiotics, while widespread disease may require oral antibiotics.
Topical antibiotics have several advantages because they are applied directly to the affected area, limiting systemic side effects. However, some patients may develop mild irritation or allergic reactions.
A Cochrane review of interventions for impetigo found that topical antibiotics are more effective than placebo for localized disease.
Mupirocin and fusidic acid are among the most effective topical treatments.
How is Mupirocin used in Impetigo?
Mupirocin ointment is commonly used to treat mild localized impetigo. It works by killing the bacteria responsible for the infection, particularly Staphylococcus aureus and Streptococcus pyogenes.
Before applying the ointment, the crusts may be gently softened using warm water and removed carefully. The medication is usually applied two to three times daily for approximately five days, depending on the severity of infection and physician recommendations.
Covering the lesions with a clean dressing may help reduce transmission and prevent scratching. Even if the sores improve rapidly, the full course of treatment should be completed.
Oral Antibiotics
Oral antibiotics may be necessary for:
- Extensive impetigo
- Bullous impetigo with multiple lesions
- Ecthyma
- Outbreaks involving several family members
- Failure of topical treatment
Studies show that cephalosporins, macrolides, and beta-lactamase–resistant penicillins are generally effective. Penicillin V and amoxicillin alone are less effective because many strains produce beta-lactamase enzymes.
Commonly used oral antibiotics include:
- Trimethoprim-sulfamethoxazole in suspected MRSA infections
- Cephalexin
- Dicloxacillin
- Amoxicillin-clavulanate
- Clindamycin
Final Word
Impetigo is an infectious and easily spread skin disease that is prevalent among the little children and in stifling conditions. Though it might appear serious, it normally only targets the outer skin, and it is very manageable provided it is detected early enough. Knowing its causes, symptoms, and types, especially, bullous and nonbullous impetigo, aid in early diagnosis as well as effective treatment. Topical antibiotics, including mupirocin, usually work but oral antibiotics can be required in infections that are more prevalent. Timely treatment and proper hygiene practices will ensure that impetigo cures in a short time and that the infection is avoided.
References
[1] Nardi, Naomi M., and Timothy J. Schaefer. “Impetigo.”PubMed, StatPearls Publishing, 31 July 2023, www.ncbi.nlm.nih.gov/books/NBK430974/.
[2] “Impetigo: Practice Essentials, Background, Pathophysiology.”Medscape.com, 13 Nov. 2019, emedicine.medscape.com/article/965254-overview.
[3] James, W. D., Elston, D. M., Treat, J. R., Rosenbach, M. A., & Neuhaus, I. M. (2020).Andrews’ diseases of the skin: Clinical dermatology(13th ed.). Elsevier.
[4] Hartman-Adams, Holly, et al. “Impetigo: Diagnosis and Treatment.”American Family Physician, vol. 90, no. 4, 2014, pp. 229–235, www.aafp.org/pubs/afp/issues/2014/0815/p229.html.
[5] Mayo Clinic. “Impetigo – Symptoms and Causes.”Mayo Clinic, 19 Apr. 2023, www.mayoclinic.org/diseases-conditions/impetigo/symptoms-causes/syc-20352352.
[6] Hartman-Adams, H., Banvard, C., & Juckett, G. (2014). Impetigo: Diagnosis and treatment.American Family Physician, 90(4), 229–235.
[7] Stevens, D. L., Bisno, A. L., Chambers, H. F., Everett, E. D., Dellinger, E. P., Goldstein, E. J. C., Gorbach, S. L., Hirschmann, J. V., Kaplan, S. L., Montoya, J. G., Wade, J. C., & Infectious Diseases Society of America. (2014).Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update.Clinical Infectious Diseases, 59(2), e10–e52. https://doi.org/10.1093/cid/ciu296
[8] Stevens, D. L., Bisno, A. L., Chambers, H. F., Everett, E. D., Dellinger, P., Goldstein, E. J. C., … Wade, J. C. (2014).Practice guidelines for the diagnosis and management of skin and soft tissue infections.Clinical Infectious Diseases, 59(2), e10–e52. https://doi.org/10.1093/cid/ciu296