
{kind=link}

Do I Feel Anxiety, that dread that sits in the chest, the sense that something is wrong even when no clear external cause is visible, is one of the scariest and most disconcerting mental health experiences. It is worse at certain times, often on waking, at night, or in the middle of an otherwise normal day. The most distressing part for most people is not the anxiety itself, but the fact that they can not identify a reason for it.
Clinicians often describe this experience as free-floating anxiety, meaning anxiety that is not linked to any specific object, person, or situation. Alongside the anxiety itself, individuals often engage in self-invalidation through an internal monologue such as, “I have no reason to feel this way,” which adds a second layer of distress.
Despite growing awareness of mental health, many people still perceive anxiety as a personality flaw or weakness, even though it reflects underlying neurological, hormonal, and psychological mechanisms that researchers can clearly identify.
What is Anxiety and Why Does it Exist?
Anxiety is the body’s internal alarm system that once kept our ancestors alive by protecting against real threats. With modern lifestyles, thoughts, memories, anticipation, and uncertainty now trigger the same system that the body originally designed to respond to physical threats.
The stress response system involves both the HPA axis (hypothalamic-pituitary-adrenal axis) and the sympathetic nervous system: when our brain perceives a threat, real or imaginary, this triggers the release of cortisol.[1] Cortisol is meant to be a short-term hormone. The body assumes that the threat will pass and hormone levels will return to the baseline. In chronic anxiety, they do not, and the body stays in a state of low-grade physiological bracing: persistent anxiety. It’s not that the brain is acting irrationally; it is simply overprotective.
Why Do I Feel Anxious For No Reason?
This is probably the most searched question in mental health. The truth is that ‘no reason’ anxiety usually has a reason, it is just not always one the person can consciously see. For example, early or subthreshold generalized anxiety symptoms can produce anxiety long before it meets the full DSM-5 diagnostic criteria for GAD.
In addition, there can be several hidden causes that a person may not realise:
- Seemingly minor stressors that don’t seem serious enough individually, but when they accumulate, can collectively overload the nervous system’s capacity.
- Sometimes internal body signals (heart rate, GI discomfort) also get misinterpreted by the brain as threat signals.
- The importance of a sound sleep is often understated; even mild chronic sleep deprivation can dysregulate the amygdala. A sleep-deprived brain has a lower threshold for perceiving neutral stimuli as threatening, so this becomes a bi-directional cycle: anxiety disturbs sleep, and poor sleep causes more anxiety.
- Blood sugar fluctuations also tend to slip under the radar, because hypoglycemia produces symptoms (tremors, sweating, racing heart) that can mimic or worsen anxiety symptoms.
- Caffeine is a well-known stimulant for cortisol and mimics the physiology of anxiety.
- Hormonal changes have direct effects on GABA receptors (the brain’s main inhibitory system), so conditions like perimenopause, PMDD, and thyroid dysfunction all produce anxiety as a symptom.[2]
- Emerging evidence links gut microbiome imbalance and GI inflammation to anxiety via the vagus nerve
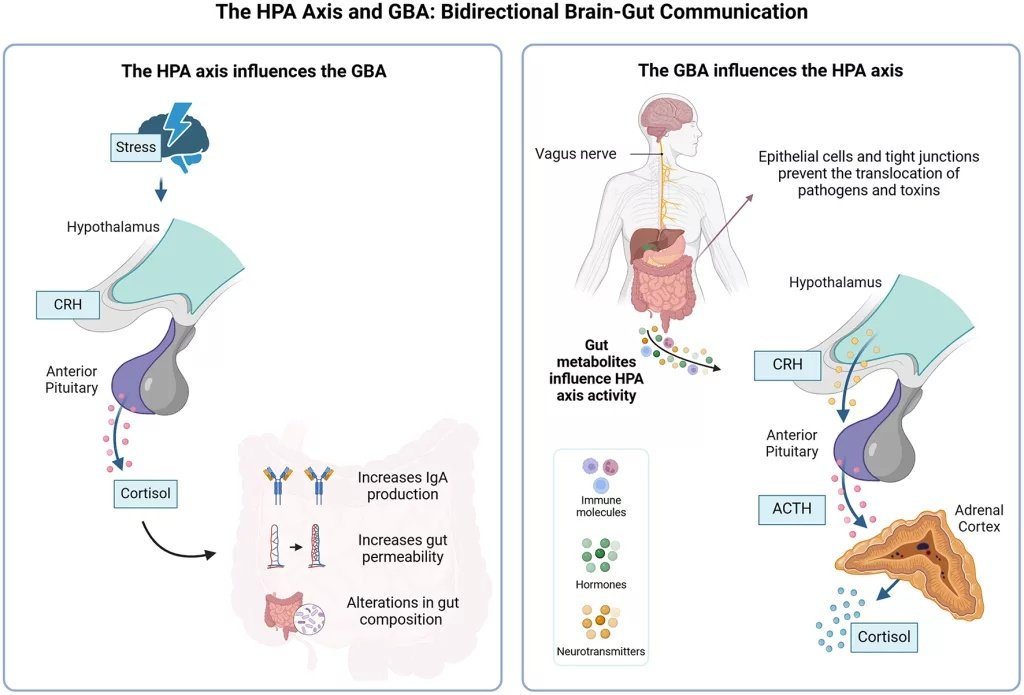
The bidirectional loop between gut health and the HPA axis: how gut dysbiosis can trigger chronic cortisol release and contribute to the physiological state of anxiety. (Image Courtesy: Bertollo AG, Santos CF, Bagatini MD, and Ignácio ZM (2025). Hypothalamus-pituitary-adrenal and gut-brain axes in the biological interaction pathway of depression. Front. Neurosci. 19:1541075. Available fromFrontiersand licensed under CC by 4.0)
Types of Anxiety Disorders
Anxiety isn’t a standalone symptom; it can be part of larger disorders, and each of these could have a different trigger:
Generalized Anxiety Disorder:
GAD is a chronic condition involving disproportionate, uncontrollable worry about multiple areas of life. The threshold for diagnosis (DSM-5) is at least 6 months of symptoms. A lot of patients who present with anxiety without a reason actually have subthreshold GAD, not long enough to be diagnosed as GAD, but not with a discernible cause either.
Panic Disorder:
Panic disorder is understood as recurrent unexpected panic attacks, which are surges of intense fear, but the surge is also associated with physical symptoms. It also comes with a persistent concern about when you might have future attacks, and this often causes a change in behavior.
Social Anxiety Disorder:
Social anxiety is the fear of scrutiny, embarrassment, or humiliation in social situations. The condition often gets misidentified as shyness, but it is actually debilitating.[3]
Specific Phobias:
There are numerous documented phobias wherein anxiety is triggered by a specific object or situation (animals, heights, blood, to name a few). These may or may not be associated with physical symptoms.
Agoraphobia:
Agoraphobia is misinterpreted as a phobia of open spaces. The clinical definition is broader: it is a fear of situations where an escape might be difficult if anxiety occurs. This includes public transport, crowds, being outside alone, and being in enclosed spaces, and it often develops secondary to panic disorder.
Illness Anxiety Disorder
Previously referred to as hypochondria or health anxiety disorder is not as widely recognised, but it is an excessive preoccupation with having or developing a serious illness, often associated with interoceptive triggers like GI discomfort.
Common Symptoms of Anxiety
Anxiety is not just a feeling; it shows up in the body, in thinking patterns, and in behavior, often in ways people do not immediately connect to anxiety. In fact, the most distressing symptoms are the ones nobody talks about: crying without knowing why, or snapping at people you love.
Physical symptoms:
Cardiovascular symptoms come first for most people, but breathing changes are also common, more so in panic attacks. These two actually feed off each other. When you notice your heart racing, it causes anxiety, which causes faster breathing, which causes more physical symptoms.
- Palpitations, tachycardia (racing heart), excessive sweating
- Dyspnoea (shortness of breath), or the sensation of not getting a full breath; this, in turn, leads to compensatory hyperventilation. Because of this hyperventilation, the CO2 levels inside the body drop, which produces the paraesthesia: tingling and numbness in the hands and around the mouth.
- Chest tightness or chest pain (often mistaken for a heart attack); the presentation can be clinically indistinguishable from angina
- Muscle tension, felt in the shoulders, neck, and the jaw (teeth grinding or bruxism is common)
- Nausea, loose stools, and IBS-like symptoms are all recognised presentations of anxiety.[4]
- Headaches, dizziness, or light-headedness
- Fatigue is very common because chronic sympathetic activation is exhausting
Cognitive Symptoms:
Anxiety also affects the way a person thinks. Most notable is the uncontrollable worry, which patients describe as being stuck in a loop they cannot exit. They also report difficulty concentrating, a constant brain fog, and intrusive, distressing thoughts. They are always scanning the surroundings for threats or repetitively replaying past events that caused distress.
Behavioral Symptoms:
- The natural human response is avoidance: that is, you start avoiding people or conditions that cause anxiety. However, though it brings immediate relief, over time, it worsens the anxiety[5]
- Sleep disturbances, difficulty falling asleep, frequent waking up, and non-restorative or restless sleep are very common in people with anxiety disorders
- Irritability is a formal DSM-5 criterion for GAD; chronic cortisol elevation lowers the amygdala’s threshold, so even minor frustrations get perceived as threats
- Crying without an apparent cause reflects dysregulation of the prefrontal cortex because of amygdala hyperactivation. Patients describe crying without knowing why or feeling emotions that seem disconnected from the actual situation. This is a recognised feature of anxiety-driven emotional dysregulation.
- Depersonalisation: feeling detached from oneself, as if watching yourself from outside your own body, often along with derealisation, such that the external world feels unreal, dreamlike, or like a film set
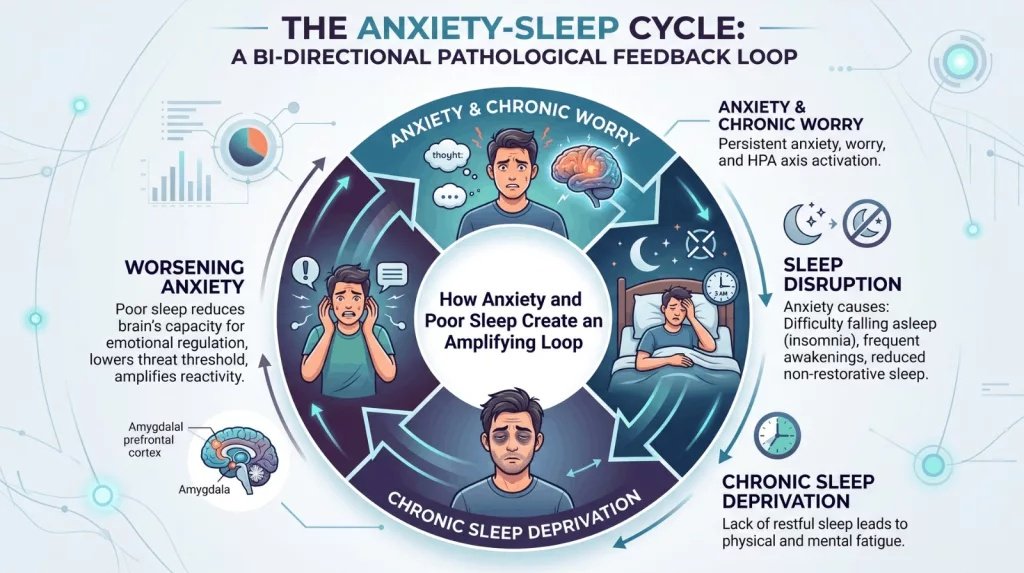
The Anxiety-Sleep Cycle:A pathological feedback loop where HPA axis activation disrupts restorative sleep, while the resulting sleep deprivation dysregulates the amygdala. This lowers the brain’s threshold for perceiving threats, effectively priming the nervous system for increased anxiety the following day.
Sometimes, anxiety doesn’t present as a clear-cut picture of these symptoms. For example, nocturnal anxiety, predominantly at night, sometimes with night sweats and vivid dreams, is a subtype that has an association with cortisol dysregulation and PTSD. High-functioning anxiety presents as emotional flatness and exhaustion rather than visible agitation.
The most underdiagnosed type, somatic anxiety, is when the patient presents to a cardiologist or gastroenterologist with physical complaints, and anxiety is never named.
Understanding What Triggers Anxiety
One of the most confusing things about anxiety is that the trigger is often not what it looks like, or there is no visible trigger at all. Triggers are not necessarily the cause, it is just what activate an already sensitized nervous system.
It can be external (situations, people, sounds) or internal (thoughts, memories, emotions, physical sensations). Internal triggers are the dominant ones in GAD and unexplained anxiety, which is why nothing outside seems to explain it.
Circadian patterns also matter: anxiety often is diurnal, worse in the morning, improving mid-day, and then sometimes worsening in the evening once again.
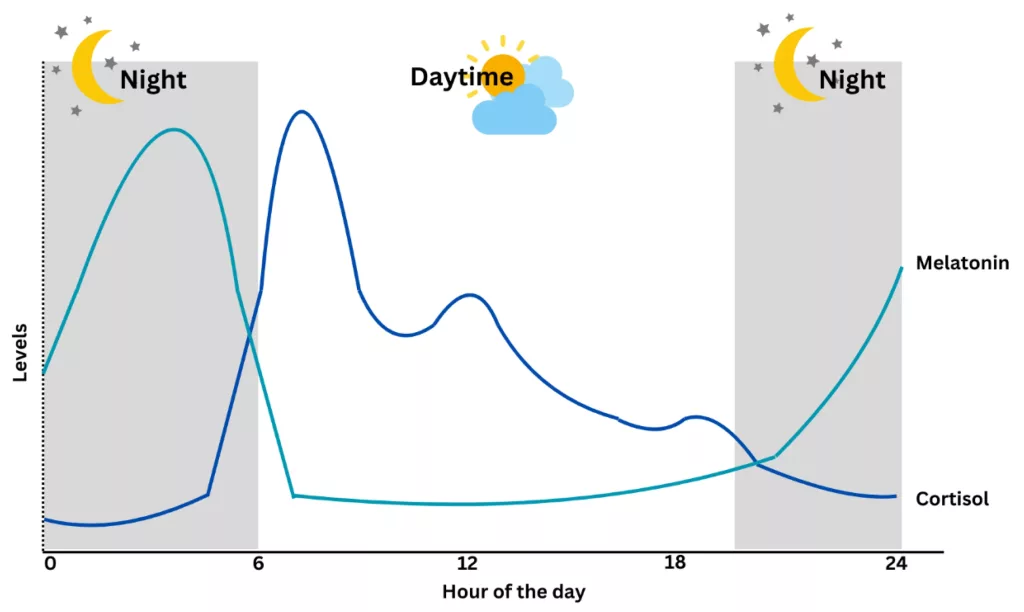
The healthy 24-hour rhythm of cortisol and melatonin: Cortisol peaks shortly after awakening to facilitate metabolic alertness and stress responsiveness, then declines during sleep. Circadian dysregulation, often influenced by light exposure, meal timing, and stress, can disrupt this pattern, potentially triggering surges of anxiety during morning or afternoon hours. (Image Courtesy: Juliana, N., Maluin, S. M., Effendy, N. M., Abu, I. F., & Azmani, S. (2025). Cortisol Detection Methods and the Hormone’s Role in Evaluating Circadian Rhythm Disruption. International Journal of Molecular Sciences, 26(18), 9141. Available fromMDPIand licensed under CC by 4.0)
When Anxiety Becomes A Medical Problem
Not all stress is anxiety, and this is an important distinction to make. There is a difference between going through a stressful period and having an anxiety disorder. Stress is a response to a specific, identifiable external trigger that resolves when the pressure is lifted. Anxiety disorder is different; it either persists even after the stress is gone or exists entirely in the absence of it, and also causes functional impairment.
Can Anxiety Be Treated?
Yes, anxiety is one of the most treatable mental health conditions; the key is to know that it won’t get better by waiting it out. In fact, leaving it untreated or avoiding it is counterproductive in that it tends to deepen over time. The goal of treatment isn’t to eliminate anxiety permanently, just to stop it from running your life. The process begins with understanding exactly what is driving the anxiety in that specific person, which is why proper assessment comes before prescription.
Diagnosing and Assessing Severity:
Clinicians diagnose anxiety disorders using DSM-5 or ICD-11 diagnostic criteria. There is no direct test or single investigation to assess anxiety directly. It requires a structured clinic process to confirm the diagnosis. The starting point is a GP or primary care clinic. Generally, the doctor takes a detailed history and examination to rule out medical conditions that can mimic anxiety (thyroid function and anemia are the most common). A structured assessment tool like the GAD-7 is used to establish severity.[6]
| Feeling, thought, or behavior | Not at all | Several days | More than half the days | Nearly every day |
|---|---|---|---|---|
| 1. Feeling nervous, anxious, or on edge | 0 | 1 | 2 | 3 |
| 2. Not being able to stop or control worrying | 0 | 1 | 2 | 3 |
| 3. Worrying too much about different things | 0 | 1 | 2 | 3 |
| 4. Trouble relaxing | 0 | 1 | 2 | 3 |
| 5. Being so restless that it is hard to sit still | 0 | 1 | 2 | 3 |
| 6. Becoming easily annoyed or irritable | 0 | 1 | 2 | 3 |
| 7. Feeling afraid as if something awful might happen | 0 | 1 | 2 | 3 |
The generalized anxiety disorder 7-item (GAD-7) scale.Scoring Guide:0–4:Minimal anxiety5–9:Mild anxiety10–14:Moderate anxiety15–21:Severe anxietySource: Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
Choosing a Treatment Strategy:
Depending on the severity determined by the GAD-7 scale, the healthcare team may refer the patient to either a psychiatrist or a psychologist. For most moderate to severe cases, a balanced approach between both works best, but for example, a very mild case would not need a drug prescription.
First-line for mild to moderate anxiety are psychological therapies, usually administered in a psychologist’s clinic once the diagnosis is made. Among these, cognitive behavioral therapy (CBT) is the gold standard.[7] Acceptance and commitment therapy (ACT), exposure therapy, and mindfulness-based approaches are strong alternatives with growing evidence.
When anxiety is moderate to severe, or when psychological therapy alone is insufficient, psychiatrists can provide medications. First-line drugs are SSRIs, but it is important to warn patients that anxiety can temporarily worsen in the first two weeks before it improves (activation syndrome), or they stop too soon.
Lifestyle changes are not optional for anxiety; aerobic exercise, sleep, and reducing caffeine intake directly affect cortisol levels and amygdala reactivity. Alcohol feels like relief in the short term, but raises the anxiety baseline over time.[8]
Takeaway
A lot of people normalize their anxiety for years because they can still function, and that shouldn’t be the threshold. If anxiety affects your sleep, relationships, goals, or any other part of your life, you should seek an assessment. A proper diagnosis does not label you; it helps explain your symptoms and equips you with tools and information to identify and manage your triggers more effectively.
References
[1] Mbiydzenyuy, N. E., & Qulu, L. A. (2024). Stress, hypothalamic-pituitary-adrenal axis, hypothalamic-pituitary-gonadal axis, and aggression. Metabolic brain disease, 39(8), 1613–1636.
[2] Albert K, Newhouse PA.Estrogen, stress, and depression: cognitive and biological interactions.Annu Rev Clin Psychol.2019;15:399–423. doi:10.1146/annurev-clinpsy-050718-095557
[3] Alomari, N. A., Bedaiwi, S. K., Ghasib, A. M., Kabbarah, A. J., Alnefaie, S. A., Hariri, N., Altammar, M. A., Fadhel, A. M., & Altowairqi, F. M. (2022). Social Anxiety Disorder: Associated Conditions and Therapeutic Approaches. Cureus, 14(12), e32687.
[4] Staudacher, H. M., Black, C. J., Teasdale, S. B., Mikocka-Walus, A., & Keefer, L. (2023). Irritable bowel syndrome and mental health comorbidity – approach to multidisciplinary management. Nature reviews. Gastroenterology & hepatology, 20(9), 582–596.
[5] Hofmann, S. G., & Hay, A. C. (2018). Rethinking avoidance: Toward a balanced approach to avoidance in treating anxiety disorders. Journal of anxiety disorders, 55, 14–21.
[6] Spitzer, R. L., Kroenke, K., Williams, J. B., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of internal medicine, 166(10), 1092–1097.
[7] David, D., Cristea, I., & Hofmann, S. G. (2018). Why Cognitive Behavioral Therapy Is the Current Gold Standard of Psychotherapy. Frontiers in psychiatry, 9, 4.
[8] Smith, J. P., & Randall, C. L. (2012). Anxiety and alcohol use disorders: comorbidity and treatment considerations. Alcohol research : current reviews, 34(4), 414–431.