
{kind=link}

Albinism is a group of heritable conditions characterized by a decrease or absence of melanin in tissues, resulting in a distinctive pale appearance. The most commonly affected tissues are ectoderm-derived, most notably skin, eyes, and hair. Melanin is a pigment produced by melanocytes that determines the color of the skin, hair, and eyes. It also plays a role in normal optic nerve and retinal development.
The term albinism originates from the word albus (white). Pathogenic variants in genes essential for melanin synthesis cause albinism. The phenotypic heterogeneity of the condition is attributed to pathogenic variants in genes that affect various stages of the melanin pathway. Most people with albinism have very pale eyes, hair, and skin. However, the colour of all three varies from person to person. People can also have vision problems. The estimated prevalence of albinism is 1 in 17,000 to 1 in 20,000. It varies by region, being higher in sub-Saharan Africa.
Causes of Albinism
Albinism is an inherited condition, as children have a chance of being born with albinism if both parents have or carry the gene for albinism. The cause of albinism is a defect in one of the several genes that produce or distribute melanin. The defect may result in the absence of melanin production or a reduction in melanin production. In most types, both parents must carry the gene, while some people with albinism have parents who are only carriers of the gene and do not show any symptoms. Ocular albinism is X-linked and typically affects individuals assigned male at birth, as the mutation is carried on the X chromosome. The specific gene mutations that cause albinism vary among different types of albinism.
Types of Albinism
There are several types of albinism based on their genetic cause. These types include:
Oculocutaneous Albinism (OCA):
It is the most common type of albinism, and people with OCA present extremely pale eyes, skin, and hair. These people also have vision problems. Seven further forms of OCA affect your body in a slightly different way.
OCA Type 1:
OCA1 occurs due to a defect in the tyrosinase enzyme.
There are two further subtypes of OCA1.
OCA1a
It occurs due to a mutation in the tyrosinase gene on chromosome 11q14, resulting in a complete lack of tyrosinase activity. People with OCA1a have a complete absence of all melanin or pigmentation. The affected individual has the most severe phenotype of all OCAs with marked hypopigmentation at birth. Individuals with this subtype often exhibit white hair, light-coloured eyes, and very pale skin.
OCA1b
OCA1B is caused by a mutation in the tyrosinase gene (TYR) on chromosome 11q14.3, resulting in reduced tyrosinase activity. This type presents with a moderate to severe phenotype. People may produce some melanin and have light-coloured eyes, hair, and skin, and the colour may increase as they age.
OCA Type 2 (OCA2):
A mutation in the OCA2 gene, located on chromosome 15q12-q13, causes this type of albinism. This mutation affects the production of the P protein.
Its presentation is less severe than OCA1. Mostly, the patients acquire small amounts of pigment with age. Patients have light brown hair and skin, and grey to tan irides.
OCA Type 3 (OCA3):
OCA3 occurs due to a mutation in tyrosinase-related protein-1 on chromosome 9p23. It usually affects dark-skinned persons. It has associations with milder vision abnormalities than other forms. Affected individuals exhibit a bright copper-red colouration of the skin and hair, as well as dilated irises.
OCA Type 4 (OCA4):
OCA4 results from mutations in the SLC45A2 (MATP) gene on chromosome 5p13. Hypopigmentation varies from mild to severe, with ocular findings characteristic of albinism.

Clinical presentation of individuals with OCA4. Image Courtesy: Oculo-Cutaneous Albinism Type 4 (OCA4): Phenotype-Genotype Correlation by Moreno-Artero, 2022,doi.org/10.3390/genes13122198, available via:https://www.mdpi.com/2073-4425/13/12/2198, CC BY 4.0.
OCA Type 5 (OCA5):
OCA5 has been mapped to chromosome 4q24, though the specific gene responsible has not yet been identified. The affected people had golden colored hair, photophobia, nystagmus, white skin, impaired visual acuity, and foveal hypoplasia.
OCA Type 6 (OCA6):
This type occurs due to a mutation in the SLC24A5 gene on chromosome 15q21. This type is observed in different ethnic groups, but was initially described in the Chinese family.
OCA Type 7 (OCA7):
OCA7 occurs due to a mutation in the C10ORF11 gene on chromosome 10q22, and affected individuals typically have predominant eye involvement, often accompanied by a light complexion.
OCA Type 8 (OCA8):
A mutation in the DCT gene, located on chromosome 13q32, causes this type of disease. It presents with mild hypopigmentation of the hair and skin, accompanied by associated ocular features.
Ocular Albinism (OA):
Ocular albinism is less common than OCA. It commonly affects your eyes rather than your skin or hair. This condition leads to blurred vision, sensitivity to light, and other symptoms that affect how you see and interact with the world around you. It is an X-linked condition that is most commonly caused by mutations in the GPR143 gene on the X chromosome (Xp22.3).
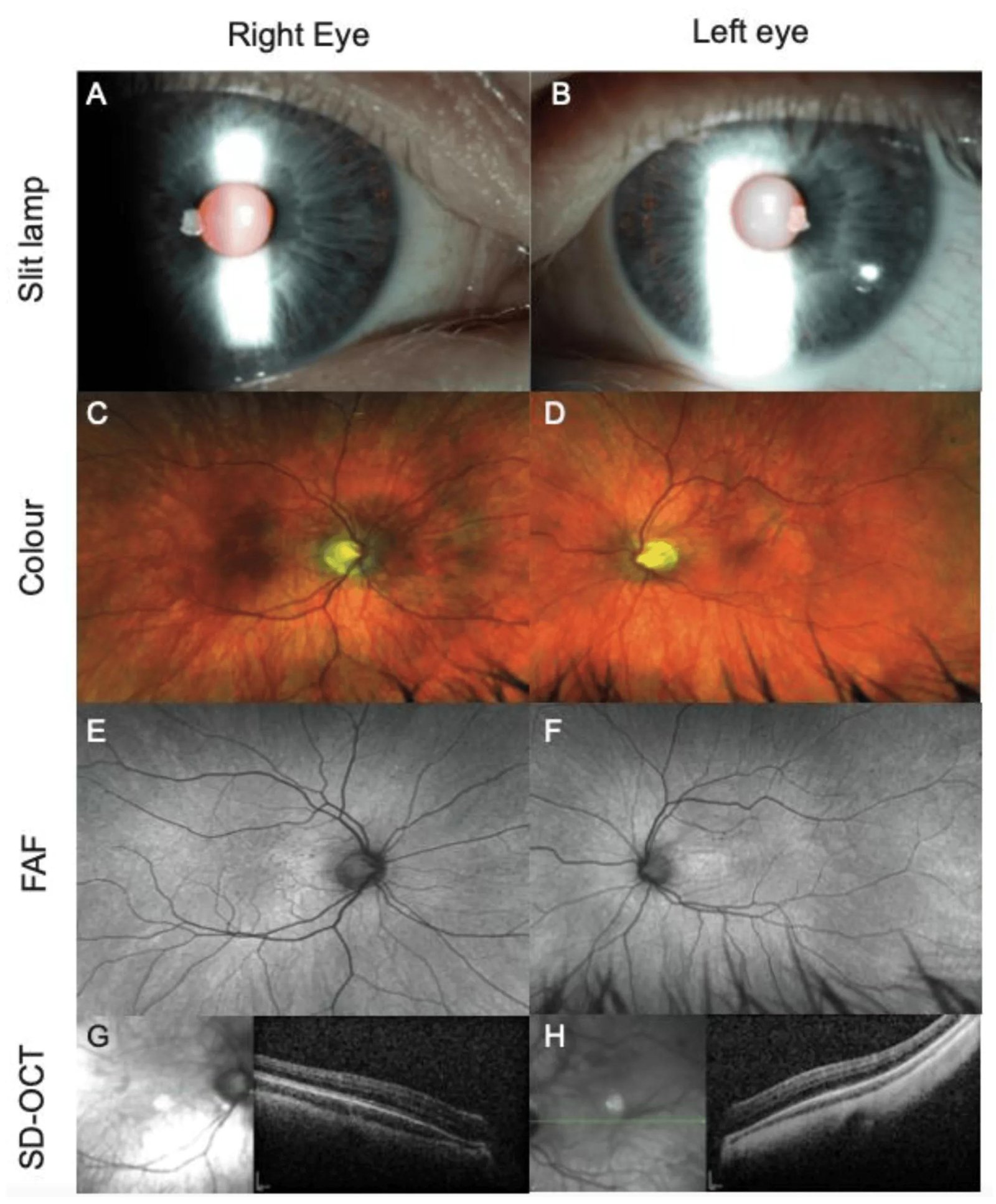
Iris and multimodal retinal imaging (right and left eye) of a patient (27079) with a homozygous TYR mutation. (A, B) Iris transillumination defects with visualization of nasal lens equator; (C, D) ultra-widefield (UWF) pseudocolor showing hypopigmented fundi and prominent choroidal vessels; (E, F) UWF fundus autofluorescence (FAF) illustrating the absence of hypoautofluoresence at the fovea due to decreased luteal pigments, crossing of retinal vessels at the fovea, and prominent choroidal vessels can be appreciated; (G, H) grade 4 foveal hypoplasia. Image Courtesy: Prospective Study of the Phenotypic and Mutational Spectrum of Ocular Albinism and Oculocutaneous Albinism by Chan et al, 2021,doi.org/10.3390/genes12040508, available via: https://www.mdpi.com/2073-4425/12/4/508, CC BY 4.0.
Hermansky-Pudlak Syndrome (HPS):
HPS is a rare form of albinism that results from mutations in any of at least 11 known genes (HPS1–HPS11, including PLDN). It produces symptoms similar to OCA. HPS is associated with platelet dysfunction causing bleeding diathesis, granulomatous colitis, and pulmonary fibrosis.
Chediak-Higashi Syndrome (CHS):
CHS is a rare form of albinism that is caused by mutations in the LYST gene, leading to defective lysosomal trafficking, which impairs immune cell function.. Its symptoms are similar to OCA. The skin colour is usually creamy white to greyish, and the hair colour is brown or blond with a silvery sheen. Additionally, people with CHS have a defect in their white blood cells, which increases the risk of infections.
Prader-Willi Syndrome (PWS) & Angelman Syndrome (AS):
Prader–Willi and Angelman syndromes are not forms of albinism but may present with hypopigmentation due to deletions affecting the OCA2 gene. Both PWS and AS occur due to spontaneous partial deletions of the long arm of chromosome 15. Specifically, AS can be caused by a deletion on the maternal chromosome. Key characteristics include severe developmental delay, ataxia, epilepsy, seizures, etc. PWS occurs due to the loss of function of genes on the paternally inherited chromosome 15. The key characteristics of PWS are hypotonia, intellectual disability, sleeping problems, and others.
Symptoms of Albinism
Symptoms appear in three areas: skin, hair, and eyes.
Skin:
People often have very pale skin. However, the exact colour varies depending on the type of albinism and the amount of melanin your body produces. For example, in OA, the skin tone is not significantly affected or is only slightly affected.
Hair:
Hair color also varies by the type of albinism. For example, individuals with OCA1 often have white hair, whereas those with other types typically have light yellow or light brown hair. Red or blond hair. The less melanin you have, the lighter your hair colour will be.
Eyes:
Most people with albinism have very pale eyes. Some may have brown or hazel eyes. Albinism not just affects the colour of your eyes, but it also affects their function and development. Hence, people with albinism can experience a wide range of eye-related symptoms.
These symptoms include:
- Photophobia (light sensitivity)
- Strabismus (crossed eyes)
- Blurry or distorted vision
- Reduced depth perception
- Refractive errors
- Nystagmus (rapid eye movements)
- Foveal hypoplasia (underdevelopment of the fovea)
- Reduced stereopsis (fine depth perception)
Diagnosis of Albinism
Early diagnosis is crucial for managing ocular symptoms and maximizing visual potential. The diagnosis of albinism involves several steps:
Physical Examination & History:
A physical examination assesses skin and hair hypopigmentation, and a thorough eye examination conducted by an ophthalmologist evaluates ocular features. History includes comparison of pigmentation with family members and review of syndromic features, such as bleeding disorders or infection, on suspicion of syndromic albinism.
Genetic Testing:
Molecular genetic testing can confirm the diagnosis. It is the most accurate method of diagnosing albinism. However, it is expensive and performed using comprehensive or multigene genome sequencing. It is particularly useful in ambiguous cases or infants where the clinical features overlap between subtypes.
No specific imaging or serological testing is required for the diagnosis of albinism. However, optical coherence tomography (OCT) can help demonstrate foveal hypoplasia.
Management & Treatment of Albinism
There is no potentially effective treatment or cure for albinism. The following options can be beneficial in enhancing the quality of life for patients with albinism. Treatment options vary depending on the affected areas.
Management of Skin Manifestations:
- The first and foremost management is lifelong sun protection.
- Healthcare providers educate patients to avoid prolonged exposure to ultraviolet light and to avoid medications that increase photosensitivity.
- People should apply sunscreen liberally and frequently (every two hours) when engaging in outdoor activities.
- Additional protection includes the use of protective clothing and eyewear, such as UV-protective sunglasses, long pants, long sleeves, UPF-labelled clothing, and hats.
Management of Eye Abnormalities:
- Tinted glasses can reduce photophobia. People need to wear dark-lensed glasses. These glasses can result in vision reduction; hence, brimmed hats can be an alternative option.
- Healthcare providers correct the refractive error with spectacle correction or contact lenses and initiate penalization or patching for amblyopia (reduced vision in one eye).
- A single device cannot serve as the solution for all patients in all situations. Young children need glasses, while older children require bifocals. For close-up work and distance vision, healthcare providers recommend bioptics (mounted on glasses).
- Healthcare providers may perform eye muscle surgery to correct strabismusif it remains unimproved despite wearing glasses. Surgery can also be an option to reduce the amplitude of nystagmus and correct head position.
Therapeutic Modalities:
There are no confirmed therapeutic modalities for albinism. However, trials are underway on these:
- Nitisinone triggers tyrosine accumulation in the blood and can improve pigmentation in OCA1b subjects in mouse models.
- Aminoglycoside readthrough therapy for nonsense mutations remains experimental.
- Adeno-associated virus vectors may be a potential gene therapy for patients with OA and OCA1.
Management of the Inheritable Nature of the Condition:
Consultation before planning a baby can be beneficial for albino parents, as albinism is an obligate homozygote condition with a full chance of passing on their defective gene. If one parent does not have albinism, then the chance of producing an albino offspring can be halved. Albino parents should undergo coordinated genetic testing to assess the likelihood of producing albino children.
Differential Diagnosis
Based on the similar cutaneous and hair findings, the differential diagnosis can include:
- Vici syndrome (an autosomal recessive disorder with absent corpus callosum. The patient may experience hypopigmentation of the skin and hair.
- Tietze albinism deafness syndrome (autosomal dominant MITF gene presenting with white eyelashes, eyebrows, and iris hypopigmentation).
- Waardenburg syndrome type II (autosomal dominant MITF gene mutation presenting with patchy skin hypopigmentation).
- Griscelli syndrome (an autosomal recessive condition presenting with hypopigmentation and silvery grey hairs).
Based on the similar ocular findings, the differential diagnosis can include:
- Hypoplasia and optic nerve atrophy
- Inherited retinal dystrophy
- Aniridia (absence of iris)
- FRMD7-related infantile nystagmus syndrome (X-linked disorder with nystagmus and reduced visual acuity)
- Cross-McKusick-Breen syndrome (an autosomal recessive disorder with hypopigmentation of skin)
- Aland Island eye disorder (X-linked disorder with fundal hypopigmentation and night blindness).
- Achromatopsia (an autosomal recessive disorder that causes dysfunctional cone cells in the retina).
Prognosis
People with non-syndromic OCA have a similar life expectancy to the general population. However, HPS and CHS can affect life expectancy due to the associated health problems. People with albinism can also limit their outdoor activities because of their eyes and skin sensitivity to the sun. UV rays can cause skin complications, including skin cancer. Additionally, poor self-image and social alienation can result in feelings of isolation and depression.
Complications
Albinism can limit work and educational opportunities due to decreased visual activities. Other complications include:
- Bleeding diathesis in HPS
- Risk of infection in CHS.
- Pachydermia
- Sola erythema
- Solar lentigines
- Actinic keratosis
- Malignancy (basal and squamous cell carcinomas)
- Melanomas
Reverse Albinism
Reverse albinism is not a formally recognized term. It can be used to refer to melanism. It is a condition characterized by an increased production of melanin. Melanism results in an unusually dark or black pigmentation of the skin and hair. It usually occurs in animal species and may provide adaptive advantages, such as UV protection or camouflage. However, it is extremely rare, if not virtually non-existent, as a natural trait in humans.
Albinism versus Leucism
Both conditions lead to reduced pigmentation, but they differ in their causes and effects. Table 1 presents a comparison of these medical conditions:
Table 1: Comparison of Albinism with Leucism
| Features | Albinism | Leucism |
|---|---|---|
| Statement | It involves a complete or near-complete absence of melanin pigment throughout the body. | It involves a partial loss or reduction of all types of pigment. |
| Causes | Genetic defects that impair melanin production enzymes, such as tyrosinase. | It occurs due to defects in the differentiation or migration of pigment-producing cells (neural crest cell), not melanin synthesis during development. |
| Affects | It causes a lack of pigment in the eyes that often results in pink or red eyes due to visible blood vessels. Pale skin and hair, vision problems. | Leucism generally does not affect eye pigmentation, so individuals have normally pigmented eyes. Patchy areas of white or pale coloration on skin or hair but not complete depigmentation. |
| Affected pigments | Melanin only | All pigment types. |
| Mechanism | In this condition, melanocytes are present, but they are unable to produce melanin. | In this condition, melanocytes are absent or reduced in the affected areas. |
| Occurrence in Humans | It occurs in humans. | It rarely occurs in humans, mostly present in animals. |
A Quick Review
Genetic conditions can be challenging to understand. Vision deficits can be a major source of debility in non-syndromic albinism. Squamous cell carcinomas and basal cell carcinomas are the most common malignancies associated with this medical condition. An international team can manage it. Whether you have had albinism for years or you get to this topic for the first time, you might feel overwhelmed. Therefore, find a healthcare provider who can explain things more clearly so you can better understand.
References
[1] Federico, J. R., & Krishnamurthy, K. (2018). Albinism.
[2] Kamaraj, B., & Purohit, R. (2013). In silico screening and molecular dynamics simulation of disease‐associated nsSNP in TYRP1 gene and its structural consequences in OCA3. BioMed research international, 2013(1), 697051.
[3] Park, S., Morya, V. K., Nguyen, D. H., Singh, B. K., Lee, H. B., & Kim, E. K. (2015). Unrevealing the role of P-protein on melanosome biology and structure, using siRNA-mediated down regulation of OCA2.Molecular and cellular biochemistry,403(1), 61-71.
[4] Kamaraj, B., & Purohit, R. (2013). In silico screening and molecular dynamics simulation of disease‐associated nsSNP in TYRP1 gene and its structural consequences in OCA3. BioMed research international, 2013(1), 697051
[5] Hayashi, M., & Suzuki, T. (2017). Oculocutaneous albinism type 4.
[6] Jung, J. H., Oh, E. H., Shin, J. H., Kim, H. S., Choi, S. Y., Choi, K. D., … & Choi, J. H. (2018). Identification of a novel GPR143 mutation in X-linked ocular albinism with marked intrafamilial phenotypic variability. Journal of genetics, 97(5), 1479-1484.
[7] S E Dorey, M. M. N., L C Burton, J J Sloper, G E Holder. (2003). The clinical features of albinism and their correlation with visual evoked potentials. British Journal of Ophthalmology, 87(6), 767-772.
[8] Sturm, V., Hejcmanova, M., & Landau, K. (2014). Effects of extraocular muscle surgery in children with monocular blindness and bilateral nystagmus. BMC ophthalmology, 14(1), 137.
[9] Prashiela Manga, S. J. O. (2011). Informed reasoning: repositioning of nitisinone to treat oculocutaneous albinism. J Clin Invest., 3828–3831.